

Sex-specific cardiometabolic multimorbidity, metabolic syndrome and left ventricular function in heart failure with preserved ejection fraction in the UK Biobank
- PMID: 40468351
- PMCID: PMC12139127
- DOI: 10.1186/s12933-025-02788-4
Sex-specific cardiometabolic multimorbidity, metabolic syndrome and left ventricular function in heart failure with preserved ejection fraction in the UK Biobank
Abstract
Background: Cardiometabolic disturbances play a central role in the pathogenesis of heart failure with preserved ejection fraction (HFpEF). Due to its complexity, HFpEF is a challenging condition to treat, making phenotype-specific disease management a promising approach. However, HFpEF phenotypes are heterogenous and there is a lack of detailed evidence on the different, sex-specific profiles of cardiometabolic multimorbidity and metabolic syndrome present in HFpEF.
Methods: We performed a retrospective, modified cross-sectional study examining a subset of participants in the UK Biobank, an ongoing multi-centre prospective cohort study in the United Kingdom. We defined HFpEF as a record of a heart failure diagnosis using ICD-10 code I50, coupled with a left ventricular ejection fraction (LVEF) ≥ 50% derived from cardiac magnetic resonance (CMR) imaging. We examined sex-specific differences in cardiometabolic comorbidity burden and metabolic syndrome, performed latent class analysis (LCA) to identify distinct clusters of patients based on their cardiometabolic profile, and compared CMR imaging-derived parameters of left ventricular function at rest in the different clusters identified to reflect possible differences in adverse cardiac remodelling.
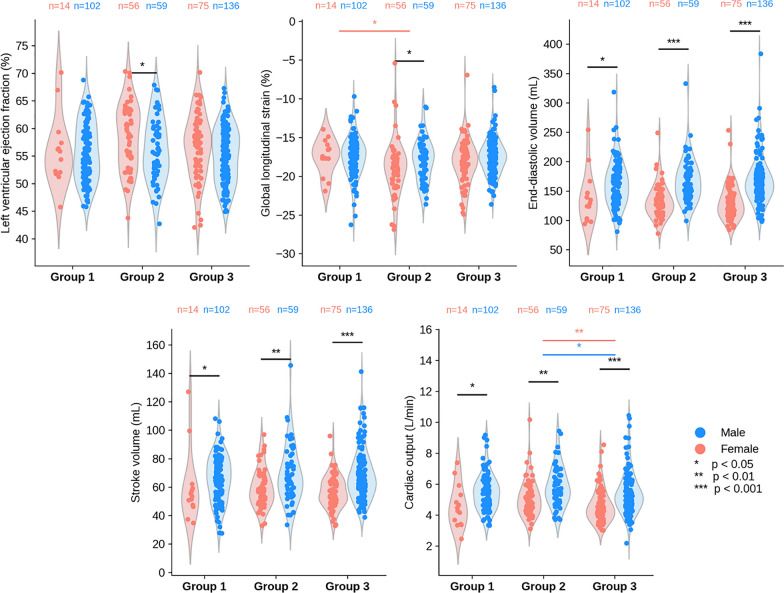
Results: We ascertained HFpEF in 445 participants, of which 299 (67%) were men and 146 (33%) women. The median age was 70 years old (interquartile range: [66.0-74.0]). A combination of hypertension and obesity was the most prevalent cardiometabolic pattern both in men and women with HFpEF. Most men had 2-3 clinical cardiometabolic comorbidities while most women had 1-2, despite a similar metabolic syndrome profile (p = 0.05). LCA revealed three distinct, clinically relevant phenogroups, namely (1) a most male and multimorbid group (n = 117); (2) a group with a high prevalence of severe obesity, abnormal waist circumference and with the highest relative proportion of females (n = 116); and finally (3) a group with an apparently lower comorbidity burden aside from hypertension (n = 212). There were significant differences in clinical measurements and medication across the three phenogroups identified. Cardiac output at rest was significantly higher in group 2 vs. group 3 (males: median 5.6 L/min vs. 5.2 L/min, p < 0.05; females: 5.1 L/min vs. 4.4 L/min, p < 0.01). Absolute global longitudinal strain was significantly lower in women in group 1 vs. group 2 (-17.6% vs. -18.5%, p < 0.05).
Conclusion: Women with cardiometabolic HFpEF had a lower comorbidity burden compared to men despite a similar metabolic syndrome profile. Based on patients' cardiometabolic profile, we identified three distinct subgroups which differed in body shape and mass, lipid biomarker and medication profile, as well as in cardiac output at rest both in men and women. These factors may affect disease trajectory, treatment options and outcomes in those subgroups. Subject to further validation, our findings provide a refined characterisation of the cardiometabolic HFpEF phenotype, contributing towards a better understanding of the condition to enable phenotype-specific disease management.
Keywords: HFpEF; UK Biobank; cardiac magnetic resonance imaging; cardiometabolic diseases; machine learning, phenomapping; metabolic syndrome.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: TM is employed by Novo Nordisk Research Centre Oxford Ltd. RG consults for Novo Nordisk A/S. TM and RG own minor Novo Nordisk company stock.
Figures


References
-
- Schiattarella GG, Alcaide P, Condorelli G, Gillette TG, Heymans S, Jones EAV, Kallikourdis M, Lichtman A, Marelli-Berg F, Shah SJ, Thorp EB, Hill JA. Immunometabolic mechanisms of heart failure with preserved ejection fraction. Nat Cardiovasc Res. 2022;1(3):211–22. 10.1038/s44161-022-00032-w. - PMC - PubMed
-
- Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, Allison M, Hemingway H, Cleland JG, McMurray JJV, Rahimi K. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018;391(10120):572–80. 10.1016/S0140-6736(17)32520-5. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
