

Chronic kidney disease prevalence and outcomes in patients with type 2 diabetes or prediabetes at high cardiovascular risk: results from the CINEMA program
- PMID: 40469223
- PMCID: PMC12133703
- DOI: 10.1016/j.ajpc.2025.101004
Chronic kidney disease prevalence and outcomes in patients with type 2 diabetes or prediabetes at high cardiovascular risk: results from the CINEMA program
Abstract
Background: Chronic kidney disease (CKD) is a global health concern, particularly among patients with type 2 diabetes mellitus (T2DM) and prediabetes who are at high risk of cardiovascular disease (CVD). The Center for Integrated and Novel Approaches in Vascular-Metabolic Disease (CINEMA) program aims to address these challenges through a multidisciplinary, patient-centered intervention. This study evaluates the CKD prevalence and outcomes in the CINEMA program, with a focus on risk for CVD and CKD progression and guideline-directed treatments.
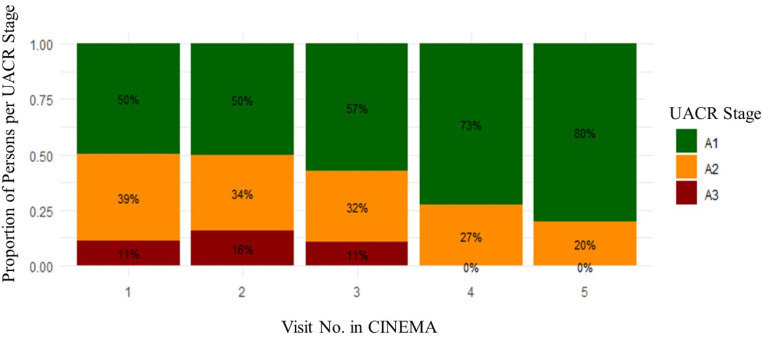
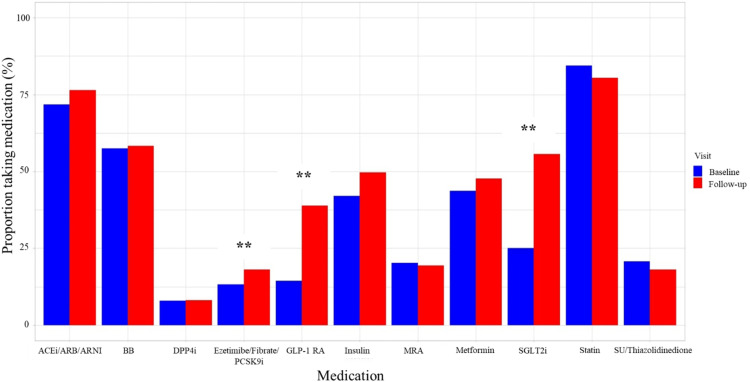
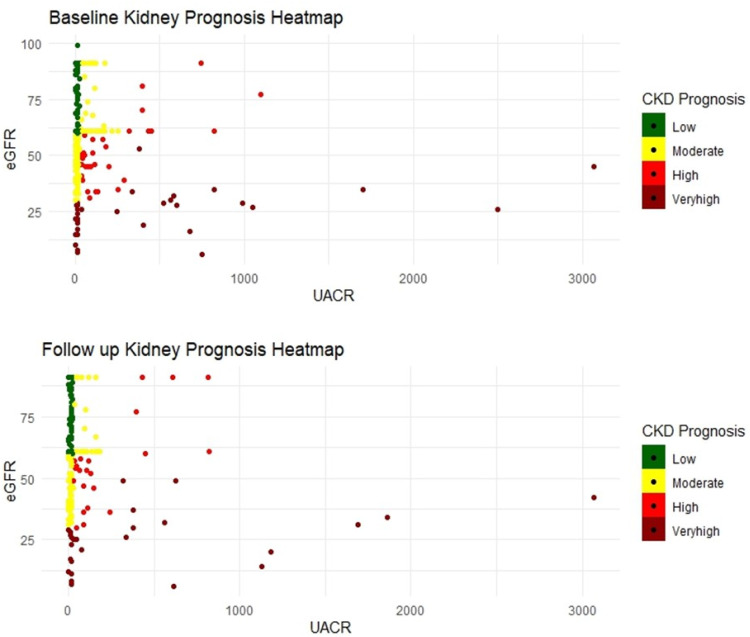
Methods and results: Patients with T2DM or prediabetes at high-risk for cardiovascular events, including those with established atherosclerotic CVD, elevated coronary artery calcium score ≥100, chronic heart failure, ischemic stroke, peripheral arterial disease, CKD (defined as eGFR<60mL/min/1.73 m and/or by the presence of urine-albumin creatinine ratio, UACR, ≥30 mg/g) and obesity with metabolic syndrome were included. From May 2020 to September 2022, 454 patients were enrolled in the CINEMA program with 45 % having a diagnosis of CKD. Among those with CKD, the median age was 64 years, 48 % were women, and 47 % were Black. 93 % had T2DM, 82 % had HTN, 52 % had established coronary artery disease, and 39 % had heart failure. Median eGFR was 49 mL/min/1.73 m and median UACR was 42 mg/g. Persons with CKD were more likely to be older, Black, have diabetes and heart failure (p < 0.05 for all). From August 2020 to June 2022, the CINEMA intervention was associated with statistically significant improvements in cardiometabolic risk factors with reductions in body weight (-3.49 lbs), BMI (-0.54 kg/m2), systolic blood pressure (-2.65 mmHg), Hb A1c (-0.63 %), total cholesterol (-9.01 mg/dL) and LDL cholesterol (-8.29 mg/dL), p < 0.05 for all. There was a trend toward lower UACR (p = 0.41) and no significant change in eGFR (p = 0.58). There was a significant increase in prescription rates of SGLT2i (25 % to 55 %) and GLP-1RA (14 % to 38 %) in the CKD population from baseline to follow-up (p < 0.05).
Conclusions: In high-risk patients with T2DM or prediabetes and CKD, the CINEMA program is effective in improving cardiovascular risk factors and shows promise in addressing CKD outcomes. Enhanced screening for CKD, appropriate risk stratification, and aggressive implementation of guideline-directed medical therapies may lead to improved long-term outcomes.
Keywords: Cardiovascular disease; Complications; Diabetes, Type 2; Health services; Quality and outcomes; Risk factors; Secondary prevention.
© 2025 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Martin S.S., Aday A.W., Almarzooq Z.I., Anderson C.A.M., Arora P., Avery C.L., Baker-Smith C.M., Barone Gibbs B., Beaton A.Z., Boehme A.K., Commodore-Mensah Y., Currie M.E., Elkind M.S.V., Evenson K.R., Generoso G., Heard D.G., Hiremath S., Johansen M.C., Kalani R., Kazi D.S., Ko D., Liu J., Magnani J.W., Michos E.D., Mussolino M.E., Navaneethan S.D., Parikh N.I., Perman S.M., Poudel R., Rezk-Hanna M., Roth G.A., Shah N.S., St-Onge M.P., Thacker E.L., Tsao C.W., Urbut S.M., Van Spall H.G.C., Voeks J.H., Wang N.Y., Wong N.D., Wong S.S., Yaffe K., Palaniappan L.P. American Heart Association Council on E, Prevention Statistics C and stroke Statistics S. 2024 Heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149:e347–e913. - PubMed
-
- Bansal N., Katz R., Robinson-Cohen C., Odden M.C., Dalrymple L., Shlipak M.G., Sarnak M.J., Siscovick D.S., Zelnick L., Psaty B.M., Kestenbaum B., Correa A., Afkarian M., Young B., de Boer I.H. Absolute rates of heart failure, coronary heart disease, and stroke in chronic kidney disease: an analysis of 3 community-based cohort studies. JAMA Cardiol. 2017;2:314–318. - PMC - PubMed
-
- Ndumele C.E., Rangaswami J., Chow S.L., Neeland I.J., Tuttle K.R., Khan S.S., Coresh J., Mathew R.O., Baker-Smith C.M., Carnethon M.R., Despres J.P., Ho J.E., Joseph J.J., Kernan W.N., Khera A., Kosiborod M.N., Lekavich C.L., Lewis E.F., Lo K.B., Ozkan B., Palaniappan L.P., Patel S.S., Pencina M.J., Powell-Wiley T.M., Sperling L.S., Virani S.S., Wright J.T., R RajgopalSingh, Elkind M.S.V., American Heart A Cardiovascular-kidney-metabolic Health: a presidential advisory from the American Heart Association. Circulation. 2023;148:1606–1635. - PubMed
-
- Pagidipati N.J., Nelson A.J., Kaltenbach L.A., Leyva M., McGuire D.K., Pop-Busui R., Cavender M.A., Aroda V.R., Magwire M.L., Richardson C.R., Lingvay I., Kirk J.K., HR Al-Khalidi, Webb L., Gaynor T., Pak J., Senyucel C., Lopes R.D., Green J.B. Granger CB and investigators CO-DS. Coordinated care to optimize cardiovascular preventive therapies in type 2 diabetes: a randomized clinical trial. JAMA. 2023;329:1261–1270. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
