

The global, regional, and national prostate cancer burden and trends from 1990 to 2021, results from the global burden of disease study 2021
- PMID: 40469596
- PMCID: PMC12133484
- DOI: 10.3389/fpubh.2025.1553747
The global, regional, and national prostate cancer burden and trends from 1990 to 2021, results from the global burden of disease study 2021
Abstract
Background: The rising annual incidence of prostate cancer (PCa) has become a significant health challenge for men worldwide. The study aims to estimate the contemporary disease burden of PCa across global, regional, and national levels.
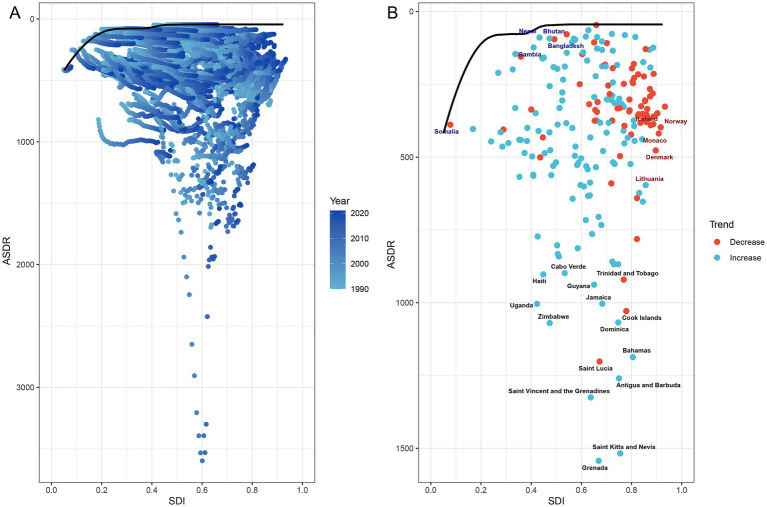
Methods: Data from the Global Burden of Disease Study 2021 (GBD 2021) was analyzed to evaluate trends in PCa incidence, prevalence, disability-adjusted life years (DALYs), and mortality from 1990 to 2021. Determinants of PCa burden were investigated through Spearman correlation analysis with socio-demographic index (SDI), decomposition analysis, and frontier analysis to assess regional improvement potential.
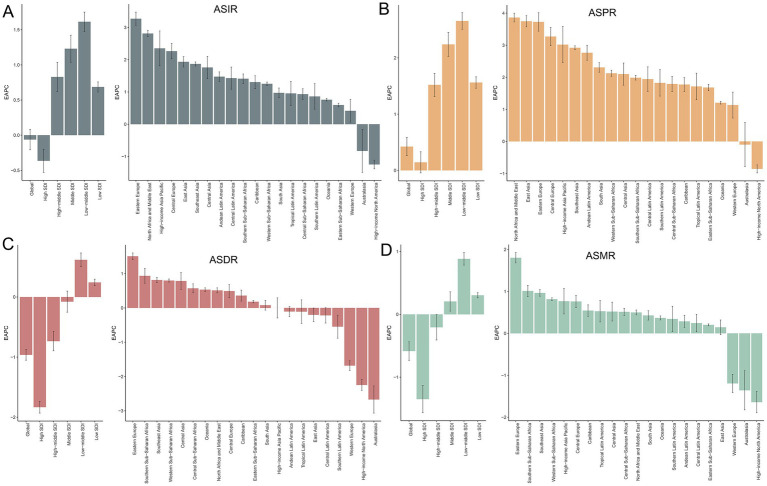
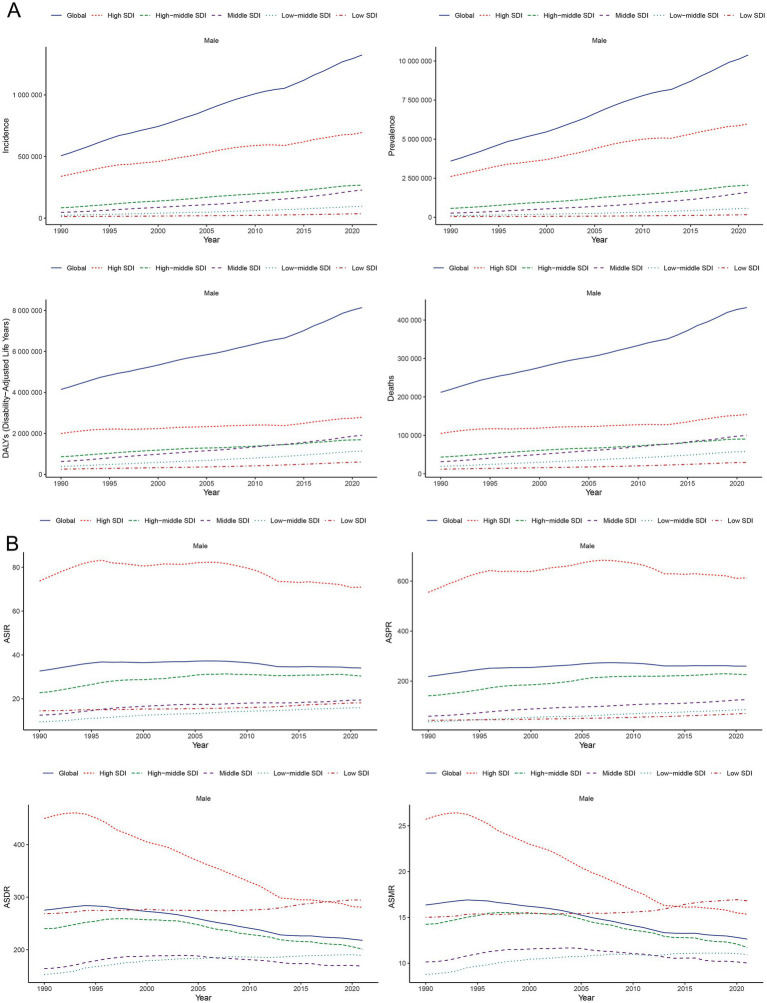
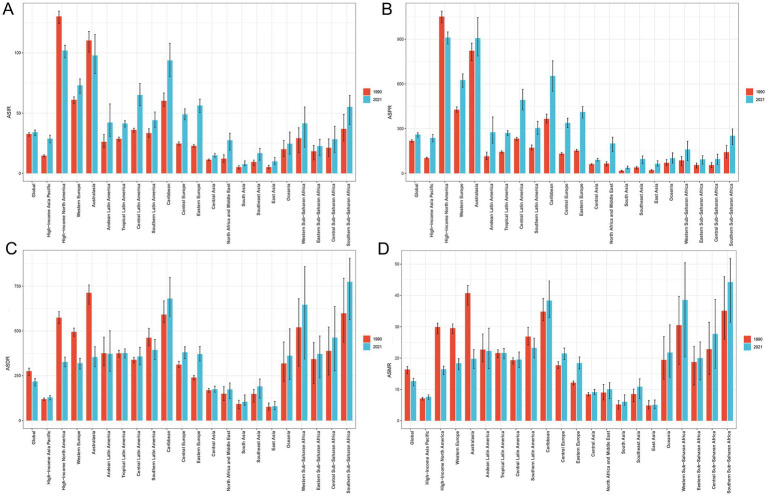
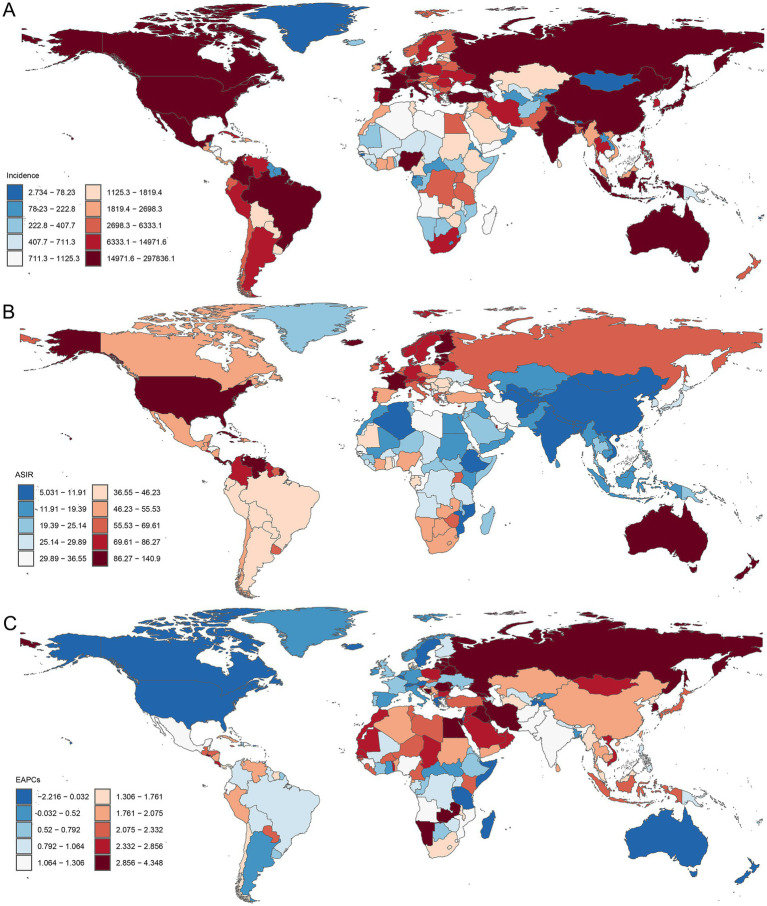
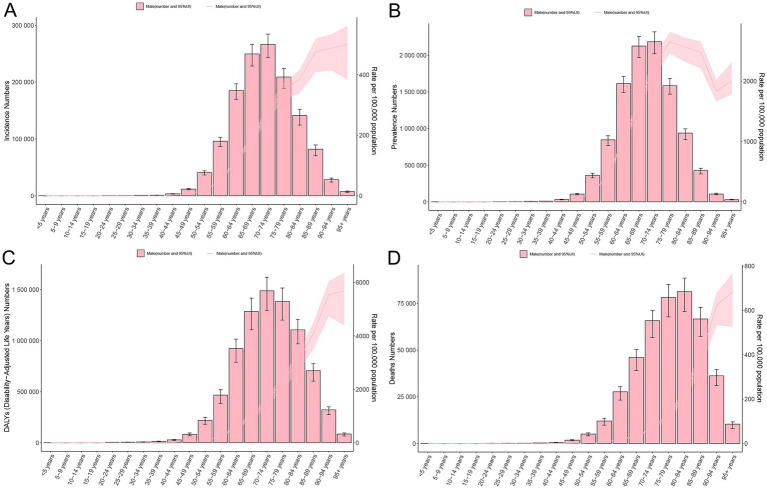
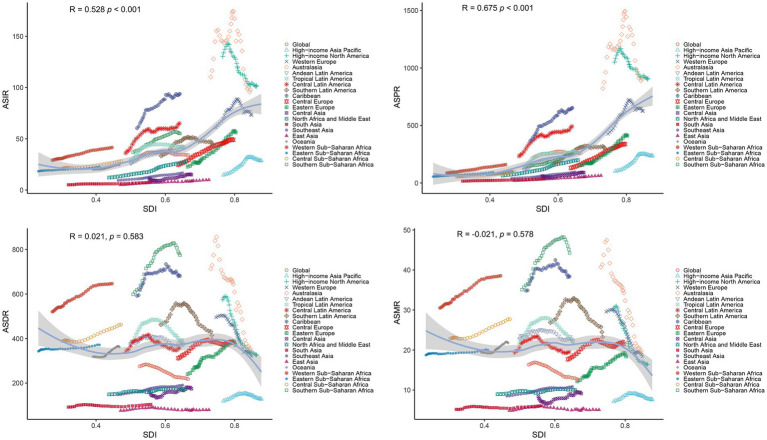
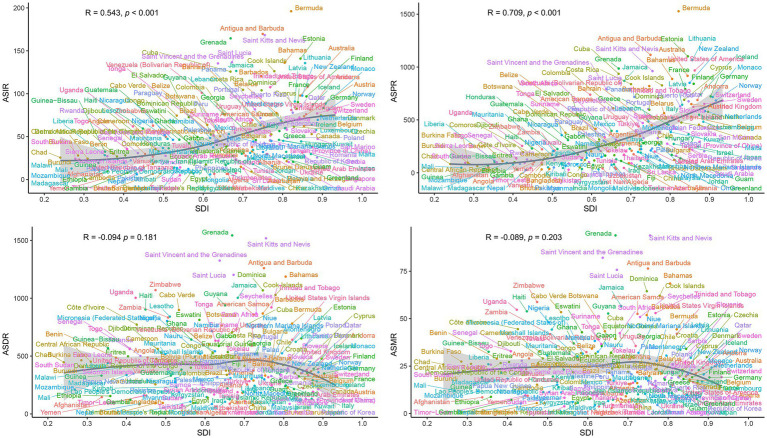
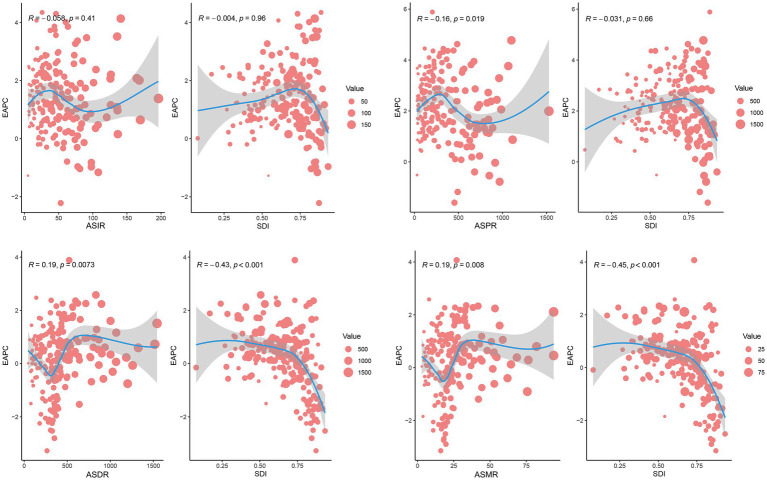
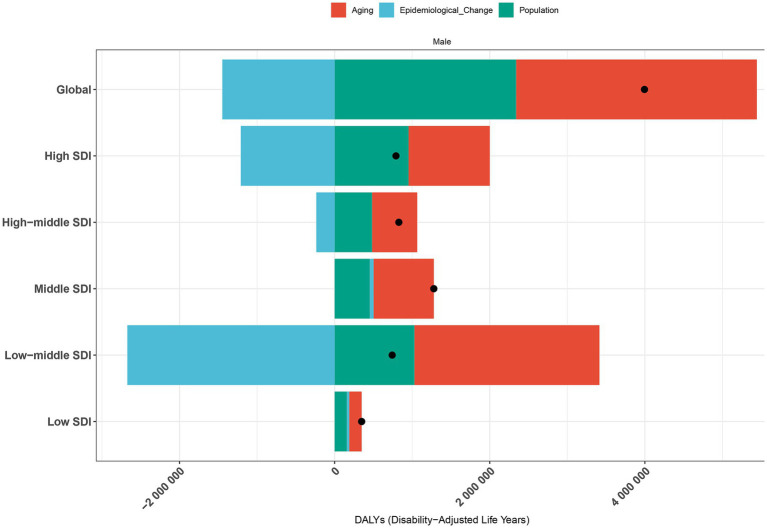
Results: In 2021, global PCa incidence reached 1.32 million cases [95% uncertainty interval (UI): 1217320.93, 1400222.17]. Between 1990 and 2021, the global estimated annual percentage change (EAPC) of age-standardized incidence rates (ASIR), prevalence rates (ASPR), DALYs rates (ASDR), and mortality rates (ASMR) were declined or increased at -0.06% [95% confidence interval (CI): -0.21, 0.08], 0.42% (95% CI: 0.26, 0.58), -0.96% (95% CI: -1.05, -0.87), and -0.58% (95% CI: -0.73, -0.44), respectively. Low-middle SDI countries exhibited the steepest rate increases, with males over 50 years being most affected. Significant positive correlations emerged between SDI levels and ASIR (R = 0.543, p < 0.001) or ASPR (R = 0.709, p < 0.001), whereas EAPC of ASDR (R = -0.430, p < 0.001) or ASMR (R = -0.450, p < 0.001) inversely correlated with SDI among 204 countries and territories. Decomposition analysis revealed the global increase of DALYs for PCa was predominantly attributed to aging (77.65%) and population growth (58.59%). Frontier analysis identified substantial improvement potential across development spectra, particularly in middle to high SDI regions.
Conclusion: Our findings demonstrated that despite modest declines in ASDR and ASMR within high SDI regions, PCa burden metrics persistently increased in low-middle SDI quintiles. Nations across all development levels require urgent implementation of evidence-based policies and precision management strategies to mitigate this growing public health challenge.
Keywords: disability-adjusted life years; global burden of disease study; incidence; mortality; prevalence; prostate cancer.
Copyright © 2025 Liu and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Zhang W, Cao G, Wu F, Wang Y, Liu Z, Hu H, et al. Global burden of prostate Cancer and association with socioeconomic status, 1990-2019: a systematic analysis from the global burden of disease study. J Epidemiol Glob Health. (2023) 13:407–21. doi: 10.1007/s44197-023-00103-6, PMID: - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical