

CD20×CD3 Bispecific Antibodies in B-NHL: A Review of Translational Science, Pharmacokinetics, Pharmacodynamics, and Dose Strategy in Clinical Research
- PMID: 40471801
- PMCID: PMC12139688
- DOI: 10.1111/cts.70250
CD20×CD3 Bispecific Antibodies in B-NHL: A Review of Translational Science, Pharmacokinetics, Pharmacodynamics, and Dose Strategy in Clinical Research
Abstract
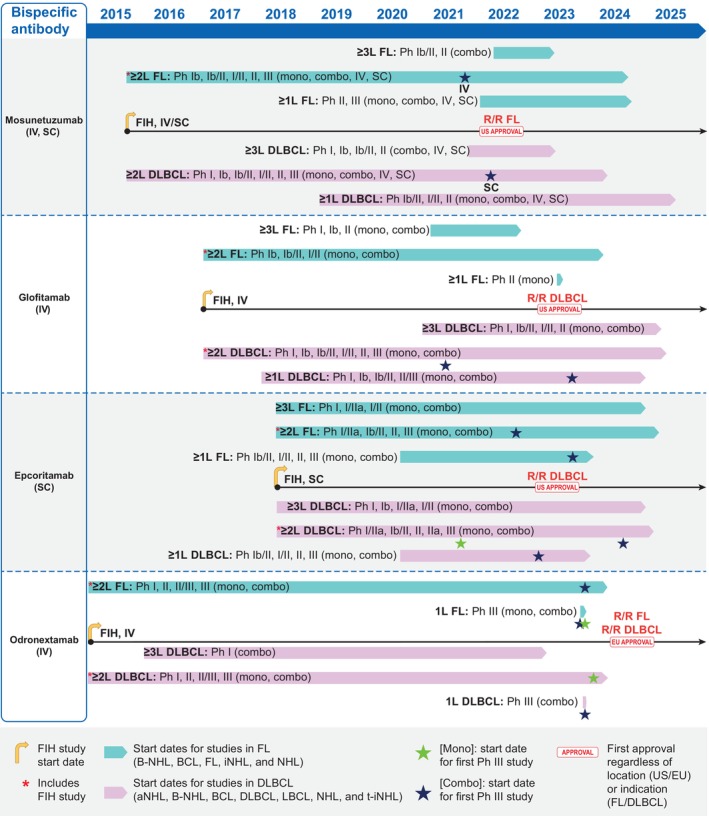
Despite advancements in treatment for B-cell non-Hodgkin lymphoma (B-NHL) in recent decades, many patients still relapse or are refractory to treatment, which represents a high unmet medical need. Novel CD20 × CD3 T-cell-engaging bispecific antibodies (bsAbs) have created a new paradigm for the treatment of B-NHL. Pivotal studies of four CD20 × CD3 bsAbs, mosunetuzumab, glofitamab, epcoritamab, and odronextamab, as monotherapy, have demonstrated robust responses with generally manageable safety profiles in patients with relapsed or refractory follicular lymphoma and diffuse large B-cell lymphoma after ≥ 2 lines of systemic therapy. These agents have presented unique challenges (e.g., cytokine release syndrome [CRS]), which have required different strategies to overcome. This review provides a comprehensive overview of the clinical development of these four CD20 × CD3 bsAbs that have been investigated for the treatment of B-NHL, with a specific focus on translational assessments to select starting doses in first-in-human studies, management of CRS, application of modeling and simulation approaches to aid dose escalation and optimization/selection, and strategies used in the design of phase I-III clinical trials. By highlighting learnings and experiences from these four bsAbs assessed, which have not been summarized collectively elsewhere, we aim to promote more efficient study design for novel bsAbs in B-NHL in the future.
Keywords: clinical trials; dose; drug development; exposure response; hematology; model‐based drug development; monoclonal antibodies; oncology; pharmacodynamics; pharmacokinetics.
© 2025 Regeneron Pharmaceuticals. Clinical and Translational Science published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
M.Z., X.G., S.G., and J.D.D. hold stock or stock options for and are employees of Regeneron Pharmaceuticals, Inc. E.W. is an employee of Orion Pharma/Orion Corporation, and an equity holder in and former employee of Regeneron Pharmaceuticals, Inc.
Figures
References
-
- Sung H., Ferlay J., Siegel R. L., et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA: A Cancer Journal for Clinicians 71, no. 3 (2021): 209–249. - PubMed
-
- Leukemia & Lymphoma Society , “NHL Subtypes,” https://www.lls.org/lymphoma/non‐hodgkin‐lymphoma/nhl‐subtypes.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
