

Polygenic scores for obstructive sleep apnoea reveal pathways contributing to cardiovascular disease
- PMID: 40472801
- PMCID: PMC12171572
- DOI: 10.1016/j.ebiom.2025.105790
Polygenic scores for obstructive sleep apnoea reveal pathways contributing to cardiovascular disease
Abstract
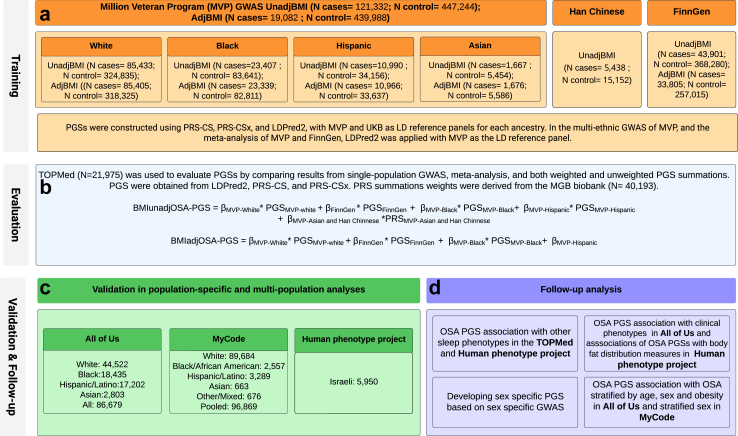
Background: Obstructive sleep apnoea (OSA) is a common chronic condition, with obesity its strongest risk factor. Polygenic scores (PGSs) summarise the genetic liability to phenotype and can provide insights into relationships between phenotypes. Recently, large datasets that include genetic data and OSA status became available, providing an opportunity to utilise PGS approaches to study the genetic relationship between OSA and other phenotypes, while differentiating OSA-specific from obesity-specific genetic factors.
Methods: Using race/ethnic diverse samples from over 1.2 million individuals from the Million Veteran Program, FinnGen, TOPMed, All of Us (AoU), Geisinger's MyCode, MGB Biobank, and the Human Phenotype Project, we developed and assessed PGSs for OSA, both without (BMIunadjOSA-PGS) and with adjustment for the genetic contributions of BMI (BMIadjOSA-PGS).
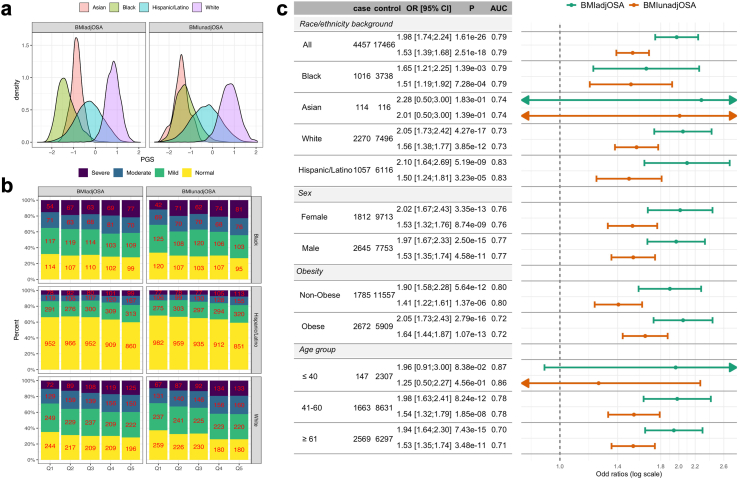
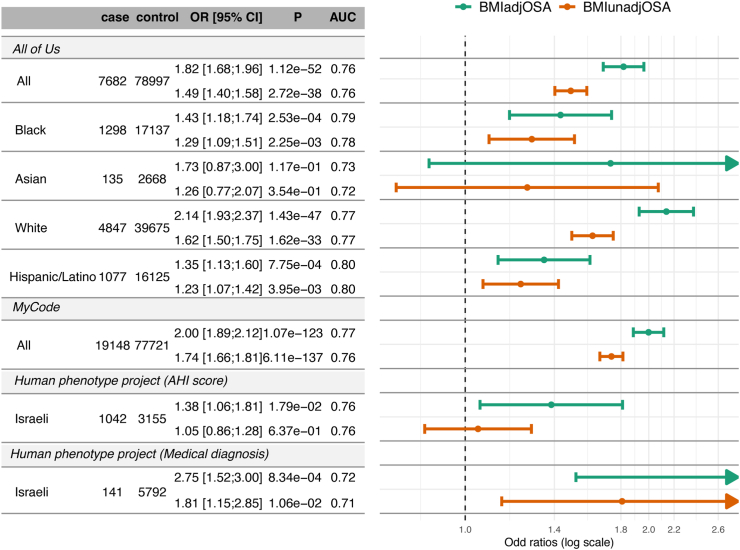
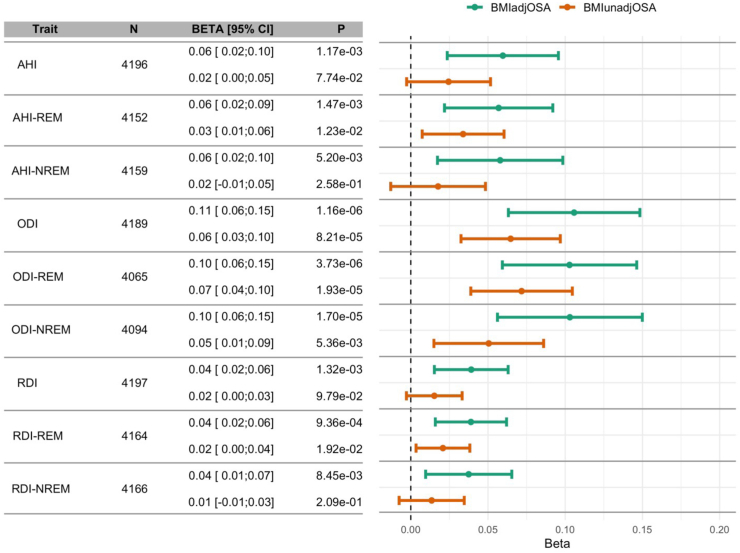
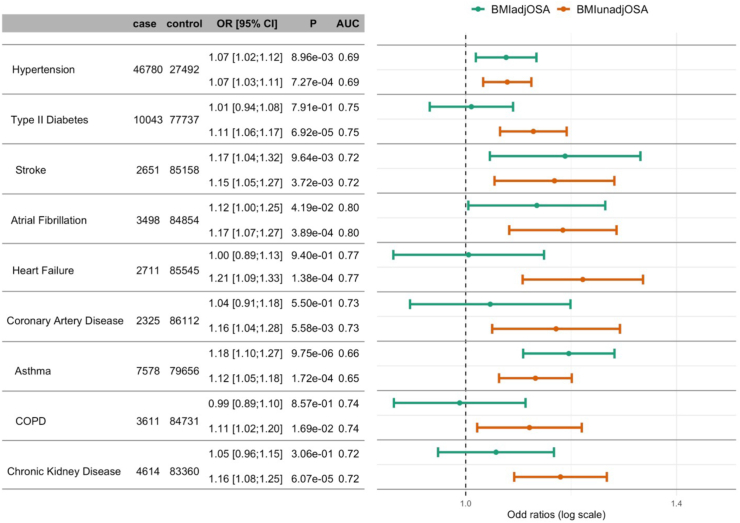
Findings: Adjusted odds ratios (ORs) for OSA per 1 standard deviation of the PGSs ranged from 1.38 to 2.75. The associations of BMIadjOSA- and BMIunadjOSA-PGSs with CVD outcomes in AoU shared both common and distinct patterns. Only BMIunadjOSA-PGS was associated with type 2 diabetes, heart failure, and coronary artery disease, while both BMIadjOSA- and BMIunadjOSA-PGSs were associated with hypertension and stroke. Sex stratified analyses revealed that BMIadjOSA-PGS association with hypertension was driven by females (OR = 1.1, p-value = 0.002, OR = 1.01 p-value = 0.2 in males). OSA PGSs were also associated with body fat measures with some sex-specific associations.
Interpretation: Distinct components of OSA genetic risk are related and independent of obesity. Sex-specific associations with body fat distribution measures may explain differing OSA risks and associations with cardiometabolic morbidities between sexes.
Funding: R01AG080598.
Keywords: Body fat distribution; Diverse populations; Genetically determined OSA; Sex differences.
Copyright © 2025 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests Dr. Cade reports receiving grants from the National Institute of Health (NIH) and from the American Academy of Sleep Medicine Foundation, and an unpaid consultancy, with a paid consulting agreement in progress through the institution, to Apnimed. Dr. Chen reports receiving consulting fees from Character Biosciences. Dr. Gottlieb reports receiving personal consulting fees from Powell Mansfield, Inc., Lilly USA, LLC, and Takeda Development Center Americas, Inc. He also reports receiving lecture honoraria from SleepRes, Inc, and from ProSomnus Sleep Technologies, and participation on a Data Safety Monitoring Board or Advisory Board for SleepRes, Inc and ProSomnus Sleep Technologies. Dr. Gupta held investment stocks of Eli Lilly (purchased in February 2024 and sold in January 2025) and of Regeneron (purchased in October 2024). Dr. Haring reports receiving lecture fees from Bristol Myers Squibb, Inari. Boehringer Ingelheim, and Pfizer, unrelated to the content of this manuscript. Dr. Keenan reports receiving support from grant P01HL160471 (Developing a P4 Medicine Approach to Obstructive Sleep Apnoea). Dr. Levy reports receiving honoraria for journal editing, as the editor in chief for IJC Cardiovascular Risk and Prevention. Dr. Moll reports receiving NIH grant K08HL159318, and a Genentech sponsored research agreement, with payments made to the institution. He also reports receiving consulting fees from 2ndMD, TheaHealth, Axon Advisors, Dialectica, Sanofi, and Verona Pharma, with payments made to him. Dr. Moll further reports payments or honoraria and travel support for lectures at the ATS 2024 and NYSTS 2024 conferences, with payments made to him. Dr. Psaty reports receiving NIH grant support, as reported in the CHS study acknowledgements, participation in the Steering Committee of the Yale Open Data Access Project, funded by Johnson & Johnson, and serving as a chair of the Board of Directors of the Am J Hypertension. Dr. Raffield reports receiving consulting fees as a consultant to the TOPMed Administrative Coordinating Center via Westat®. Dr. Redline reports receiving consulting fees from Eli Lilly, related to work on GLP-1 and OSA, with payments made to her. Dr. Rich reports receiving consulting fees from Westat, as a consultant to the Administrative Coordinating Center for the NHLBI Trans-Omics for Precision Medicine program. Dr. Rotter reports NIH grant support. Dr. Sofer reports grant support from the National Institute on Aging and from the National Heart Lung and Blood Institute, with payments made to the institution.
Figures


References
-
- Mokhlesi B., Ham S.A., Gozal D. The effect of sex and age on the comorbidity burden of OSA: an observational analysis from a large nationwide US health claims database. Eur Respir J. 2016;47(4):1162–1169. - PubMed
-
- Bradley T.D., Floras J.S. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82–93. - PubMed
-
- Marin J.M., Carrizo S.J., Vicente E., Agusti A.G.N. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053. - PubMed
-
- Kapur V., Strohl K.P., Redline S., Iber C., O'Connor G., Nieto J. Underdiagnosis of sleep apnea syndrome in U.S. communities. Sleep Breath. 2002;6(2):49–54. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
