

Psilocybin's acute and persistent brain effects: a precision imaging drug trial
- PMID: 40473634
- PMCID: PMC12141498
- DOI: 10.1038/s41597-025-05189-0
Psilocybin's acute and persistent brain effects: a precision imaging drug trial
Erratum in
-
Correction: Psilocybin's acute and persistent brain effects: a precision imaging drug trials.Sci Data. 2025 Jun 18;12(1):1029. doi: 10.1038/s41597-025-05397-8. Sci Data. 2025. PMID: 40533500 Free PMC article. No abstract available.
Abstract
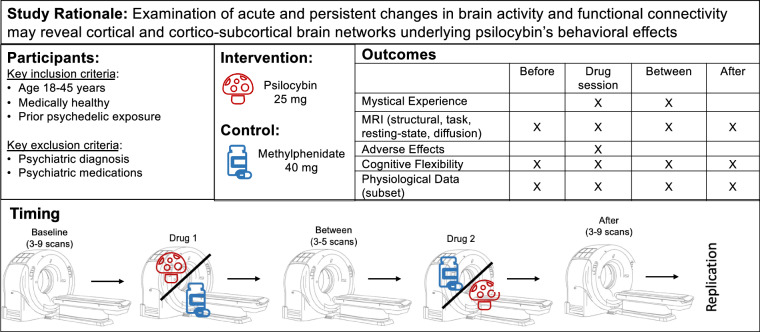
Psilocybin (PSIL) is a psychedelic drug and a promising experimental therapeutic for many psychiatric conditions. Precision functional mapping (PFM) combines densely repeated resting state fMRI sampling and individual-specific network mapping to improve signal-to-noise ratio (SNR) and effect size in brain imaging research. We present a randomized cross-over study in which PFM was used to characterize acute and persistent effects of psilocybin or methylphenidate (MTP) on brain networks. Seven healthy volunteers (mean age 34.1 years, SD = 9.8; n = 3 females, n = 6 Caucasians) underwent (1) extensive baseline imaging, (2) imaging beginning 60-90 minutes after drug exposure, and (3) longitudinal imaging for up to two weeks after drug exposure. Four individuals also participated in an open-label PSIL replication protocol over 6 months later. This dataset includes resting state (using advanced high-resolution multi-echo fMRI), task fMRI, structural, and diffusion basis spectral imaging as well as assessments of subjective experience. We are releasing this unique dataset as a resource for neuroscientists to study the acute and persistent effects of PSIL and MTP on brain networks.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Within the last two years, author JSS was an employee of Sumitomo Pharma America and received consulting fees from Longitude Capital. Author GEN has served as principal or co-investigator on studies funded by Alkermes, Inc., LB Pharmaceuticals and COMPASS Pathways, and has received research support from Usona Institute (drug only). She has served as a paid consultant for Carelon and Alkermes, Inc. AZS is a consultant for Soraneuroscience, LLC. NUFD is a co-founder of Turing Medical Inc, and may benefit financially if the company is successful in marketing FIRMM motion monitoring software products and may receive royalty income based on FIRMM technology developed at Washington University School of Medicine (WUSOM) and licensed to Turing Medical Inc.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
- U01 DA041120/DA/NIDA NIH HHS/United States
- MH129616/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- K23 NS088590/NS/NINDS NIH HHS/United States
- MH096773/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- DA007261/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- R00 MH129616/MH/NIMH NIH HHS/United States
- T32 DA007261/DA/NIDA NIH HHS/United States
- R44 MH121276/MH/NIMH NIH HHS/United States
- NS129521/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- MH122066/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- K99 MH129616/MH/NIMH NIH HHS/United States
- MH112473/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- MH121276/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- R25 MH112473/MH/NIMH NIH HHS/United States
- R01 MH096773/MH/NIMH NIH HHS/United States
- R44 NS129521/NS/NINDS NIH HHS/United States
- MH124567/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- NS088590/U.S. Department of Health & Human Services | NIH | National Institute of Mental Health (NIMH)
- R44 MH124567/MH/NIMH NIH HHS/United States
- R44 MH122066/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
