

Multimodal assessment of sleep-wake perception in insomnia disorder
- PMID: 40473645
- PMCID: PMC12141479
- DOI: 10.1038/s41598-025-00995-3
Multimodal assessment of sleep-wake perception in insomnia disorder
Abstract
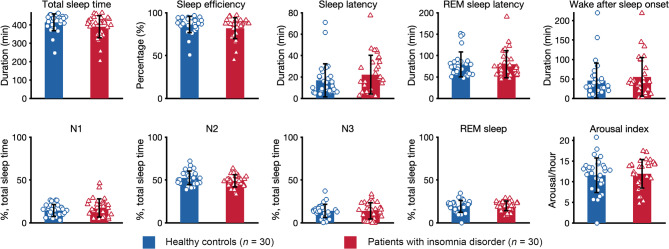
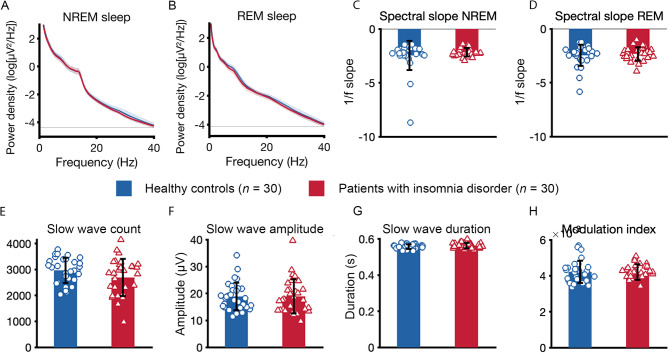
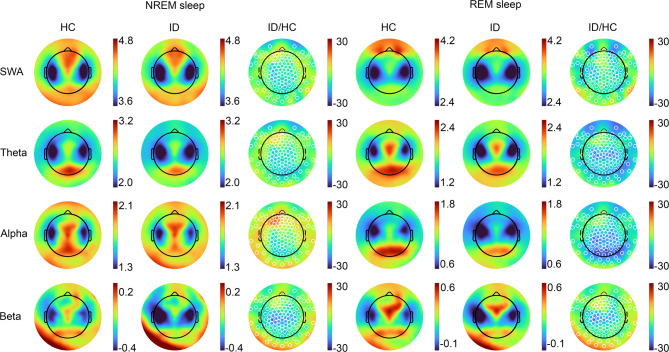
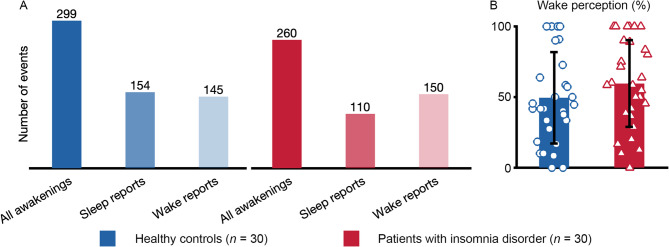
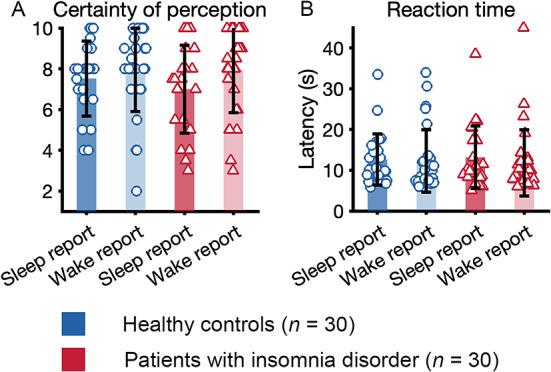
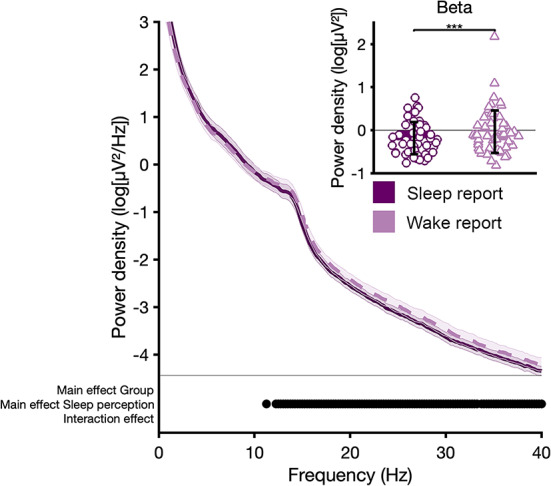
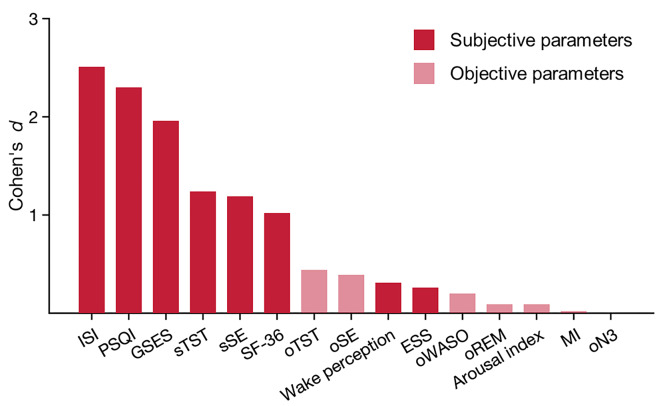
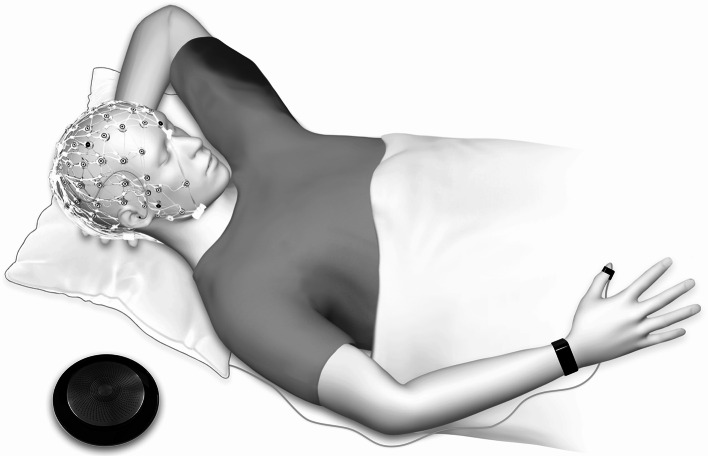
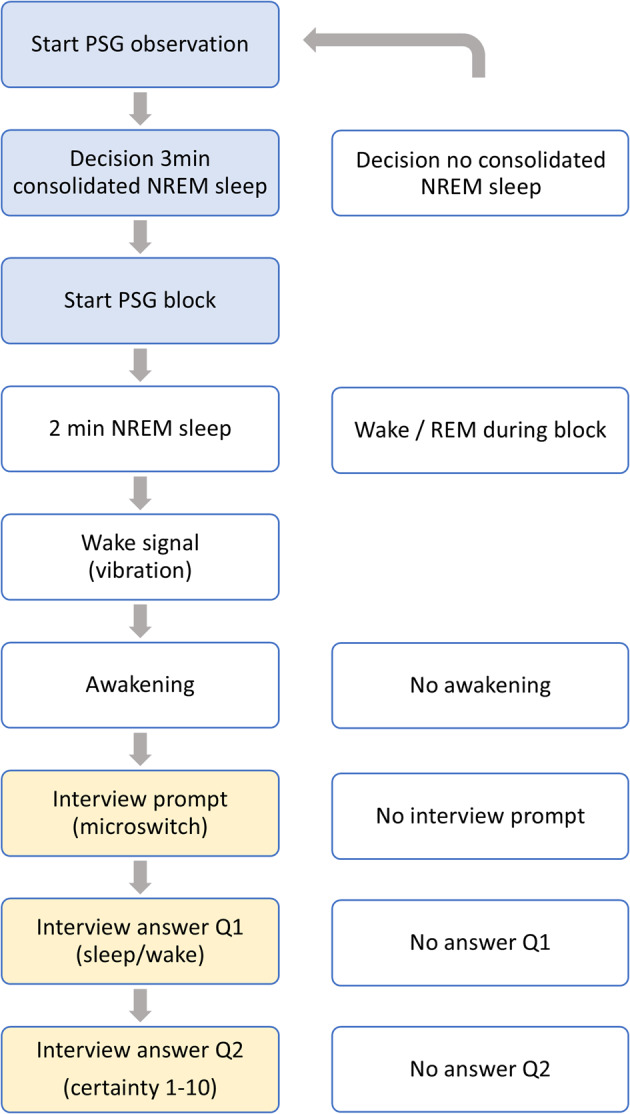
Insomnia disorder is a prevalent health problem. The primary diagnostic criterion is a subjective complaint about reduced quantity or quality of sleep, which is often not observed in objective sleep measurements. Here we show that patients with insomnia disorder, characterized by substantial subjective sleep complaints, did not differ on objective measures of sleep continuity, sleep architecture, spectral power, spectral slope, and phase-amplitude coupling of slow oscillatory and spindle activity. Perception of wakefulness following serial awakenings from NREM sleep was frequent in both patients and controls, with no significant group difference. High frequency spectral power, as an index of cortical arousal prior to awakening, but not standard measures of sleep, predicted the perception of wakefulness across groups, possibly related to physiological wake-like activity during sleep. Our results support the notion that sleep-wake regulatory systems and direct sleep-wake perception are often intact in patients with insomnia disorder. These results propose empirical support for cognitive behavioral therapy for insomnia as the first-line treatment.
Keywords: Insomnia disorder; Polysomnography; Serial awakening; Sleep-wake perception; Spectral analysis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: C.N. has served on advisory boards of Janssen, Idorsia and the GetOn Institute. All other authors declare no competing interests.
Figures
Similar articles
-
Insomnia disorder is associated with 24-hour cortical hyperarousal.Sleep Med. 2024 Dec;124:681-687. doi: 10.1016/j.sleep.2024.11.002. Epub 2024 Nov 9. Sleep Med. 2024. PMID: 39536528
-
The subjective-objective mismatch in sleep perception among those with insomnia and sleep apnea.J Sleep Res. 2013 Oct;22(5):557-68. doi: 10.1111/jsr.12046. Epub 2013 Mar 25. J Sleep Res. 2013. PMID: 23521019
-
Insomnia-perchance a dream? Results from a NREM/REM sleep awakening study in good sleepers and patients with insomnia.Sleep. 2018 May 1;41(5). doi: 10.1093/sleep/zsy032. Sleep. 2018. PMID: 29432570
-
(Mis)perception of sleep in insomnia: a puzzle and a resolution.Psychol Bull. 2012 Jan;138(1):77-101. doi: 10.1037/a0025730. Epub 2011 Oct 3. Psychol Bull. 2012. PMID: 21967449 Free PMC article. Review.
-
Insomnia and sleep misperception.Pathol Biol (Paris). 2014 Oct;62(5):241-51. doi: 10.1016/j.patbio.2014.07.003. Epub 2014 Aug 29. Pathol Biol (Paris). 2014. PMID: 25179115 Review.
Cited by
-
Nutritional and Lifestyle Behaviors and Their Influence on Sleep Quality Among Spanish Adult Women.Nutrients. 2025 Jul 4;17(13):2225. doi: 10.3390/nu17132225. Nutrients. 2025. PMID: 40647329 Free PMC article.
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. American Psychiatric Association. (2013). 10.1176/appi.books.9780890425596
-
- American Academy of Sleep Medicine, ed. International Classification of Sleep Disorders 3. edn (American Acad. of Sleep Medicine, 2014).
-
- World Health Organization (WHO). International Classification of Diseases, Eleventh Revision (ICD-11), (2019).
-
- Riemann, D. et al. The European insomnia guideline: an update on the diagnosis and treatment of insomnia 2023. J. Sleep. Res.32 (6), e14035. 10.1111/jsr.14035 (2023). - PubMed
-
- Baglioni, C. et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 135 (1–3), 10–19. 10.1016/j.jad.2011.01.011 (2011). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
