

Comparative assessment of seven surgical procedures in Carpal Tunnel Syndrome: a network meta-analysis empowering physician-patient decision-making
- PMID: 40473869
- PMCID: PMC12141404
- DOI: 10.1007/s10143-025-03587-x
Comparative assessment of seven surgical procedures in Carpal Tunnel Syndrome: a network meta-analysis empowering physician-patient decision-making
Abstract
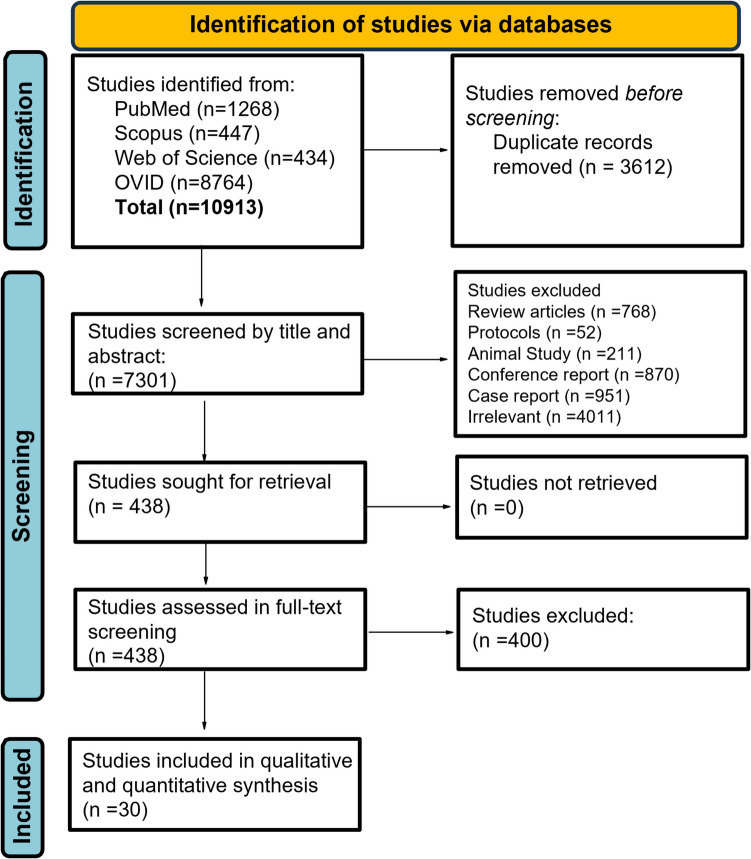
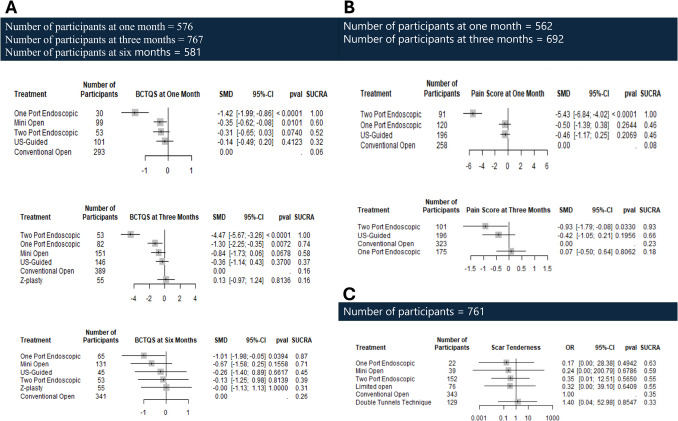
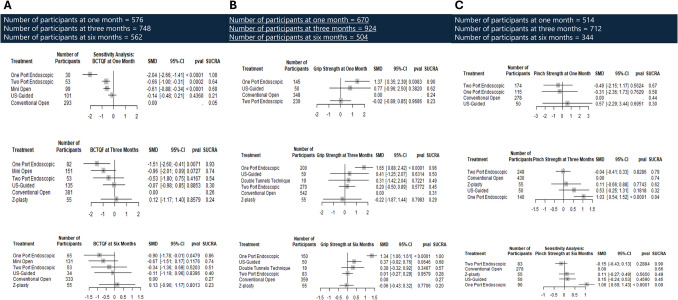
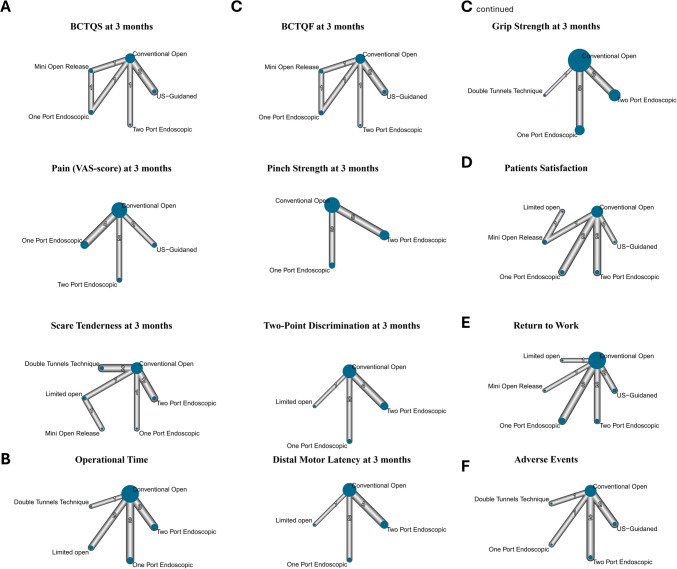
Carpal Tunnel Syndrome (CTS) is a common peripheral nerve entrapment disorder with a high global burden. Various surgical techniques have been developed to optimize symptom relief and minimize postoperative morbidity. This network meta-analysis (NMA) aimed to compare the relative efficacy and safety of different carpal tunnel release (CTR) procedures. We conducted a systematic review and NMA of randomized controlled trials (RCTs) comparing surgical CTR techniques. Outcomes included symptom severity, pain scores, functional status, patient-reported outcomes, operative time, and adverse events. Data were synthesized using the frequentist approach with the netmeta package in R. Confidence in network estimates was evaluated using the CINeMA framework. Thirty-two RCTs comprising 2,916 patients were included. One-port and two-port endoscopic CTR (ECTR) techniques demonstrated superior symptom relief compared to conventional open CTR (COCTR), particularly at three months (two-port ECTR: SMD = -4.47; 95% CI: -5.67 to -3.26). One-port ECTR consistently showed better functional outcomes across all timepoints, including improved grip (SMD = 1.37; 95% CI: 0.35 to 2.39) and pinch strength. Pain was significantly reduced with two-port ECTR at one and three months. Ultrasound-guided CTR (CTR-US) showed the highest patient satisfaction (OR = 6.89; 95% CI: 1.87 to 25.43) and a significantly shorter return-to-work duration. The double tunnels technique (DTT) had the lowest risk of adverse events (OR = 0.05; 95% CI: 0.01 to 0.42). Operational time and scar tenderness were comparable across all techniques. Heterogeneity was generally low to moderate across outcomes, and CINeMA assessments indicated moderate to low confidence in several comparisons. Endoscopic techniques, particularly one- and two-port ECTR, offer superior outcomes in symptom severity and functional recovery compared to COCTR. CTR-US appears to maximize patient satisfaction and early return to work, while DTT is associated with the fewest complications. These findings can guide individualized, evidence-based treatment decisions in CTS surgery.
Keywords: Carpal tunnel syndrome; Conventional open carpal tunnel release; Double tunnel release; Endoscopic carpal tunnel release; Ultrasound-guided carpal tunnel release (CTR-US).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors. Disclosure: None of the authors received payments or services via his or her institution or from third parties. Informed consent: No informed consent is required for this study design. Consent for publication: All authors'consent has been obtained by the corresponding author for publication. Competing interest: The authors declare no competing interests.
Figures

References
-
- Graham B, Peljovich AE, Afra R, Cho MS, Gray R, Stephenson J, Gurman A, MacDermid J, Mlady G, Patel AT et al (2016) The American Academy of Orthopaedic Surgeons Evidence-Based Clinical Practice Guideline on: Management of Carpal Tunnel Syndrome. J. Bone Joint Surg. Am. 98:1750–1754. 10.2106/JBJS.16.00719 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
