

Effectiveness and analgesic effect of local infiltration analgesia and femoral nerve block after anterior cruciate ligament reconstruction: a systematic review and meta-analysis
- PMID: 40474133
- PMCID: PMC12142901
- DOI: 10.1186/s12891-025-08665-1
Effectiveness and analgesic effect of local infiltration analgesia and femoral nerve block after anterior cruciate ligament reconstruction: a systematic review and meta-analysis
Abstract
Background: Anterior cruciate ligament reconstruction (ACLR) is frequently associated with moderate to severe postoperative pain, necessitating effective analgesic strategies to enhance patient comfort and facilitate recovery. Identifying effective pain management methods after ACLR is crucial. This study aims to explore the best analgesia method with the local infiltration analgesia (LIA) and femoral nerve block (FNB) after ACLR.
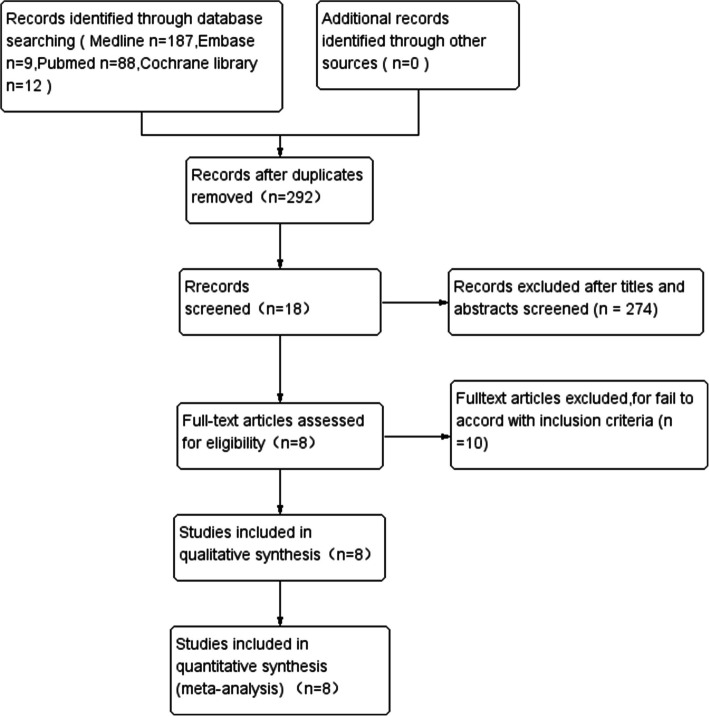
Methods: Cochrane Library databases, PubMed, MEDLINE and Embase were searched from inception to April 2024 with the following terms: "anterior cruciate ligament" AND "reconstruction" AND "femoral nerve block" AND "local infiltration analgesia" AND "pain score" AND "morphine consumption" AND "analgesia duration" AND "complication".
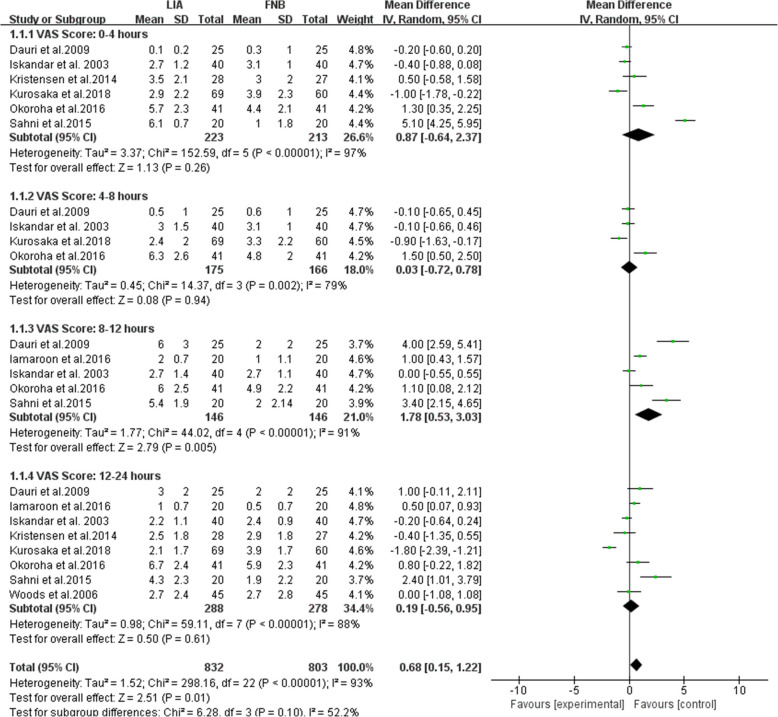
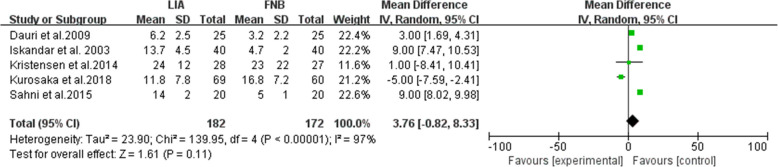
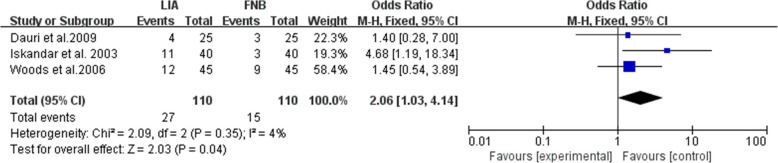
Results: A total of 8 Level 1 randomized controlled trials (RCTs) were included in Meta analysis. The pain score of the FNB group was significantly lower than that of the LIA group at 8 to 12 h after the operation (MD = 1.78; 95% CI, [0.53, 3.03]; P = 0.005). There was no significant difference in pain scores between the two groups at 0 to 4, 4 to 8, and 12 to 24 h postoperatively. Within 24 h after surgery, there was no significant difference in intravenous morphine equivalent consumption between the two groups (MD = 3.76; 95% CI, [-0.82, 8.33]; P = 0.11). In terms of analgesic duration, there was also no significant difference between the two groups (MD = -3.03; 95% CI, [-7.34, 1.28]; P = 0.17). However, the incidence of nausea in the LIA group was higher than that in the FNB group (OR = 2.06; 95% CI, [1.03, 4.14]; P = 0.04).
Conclusion: The FNB is superior to LIA for intraoperative control of postoperative pain in the first 8 to 12 h after ACLR. But there was no significant difference in pain control at other time points, morphine consumption, and analgesic duration between the two groups within 24 h after surgery. The LIA group had a higher incidence of nausea within 24 h after surgery.
Keywords: Anterior cruciate ligament reconstruction; Femoral nerve block; Local infiltration analgesia; Pain.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Combined femoral and sciatic nerve block versus femoral and local infiltration anesthesia for pain control after total knee arthroplasty: a meta-analysis of randomized controlled trials.J Orthop Surg Res. 2016 Dec 7;11(1):158. doi: 10.1186/s13018-016-0495-6. J Orthop Surg Res. 2016. PMID: 27923404 Free PMC article.
-
Is Local Infiltration Analgesia Superior to Peripheral Nerve Blockade for Pain Management After THA: A Network Meta-analysis.Clin Orthop Relat Res. 2016 Feb;474(2):495-516. doi: 10.1007/s11999-015-4619-9. Epub 2015 Nov 16. Clin Orthop Relat Res. 2016. PMID: 26573322 Free PMC article.
-
The efficacy of local infiltration analgesia in the early postoperative period after total knee arthroplasty: A systematic review and meta-analysis.Eur J Anaesthesiol. 2016 Nov;33(11):816-831. doi: 10.1097/EJA.0000000000000516. Eur J Anaesthesiol. 2016. PMID: 27428259
-
Comparison of local infiltration analgesia and sciatic nerve block for pain control after total knee arthroplasty: a systematic review and meta-analysis.J Orthop Surg Res. 2017 Jun 7;12(1):85. doi: 10.1186/s13018-017-0586-z. J Orthop Surg Res. 2017. PMID: 28592324 Free PMC article.
-
Intrathecal morphine verse femoral nerve block for pain control in total knee arthroplasty: A meta-analysis from randomized control trials.Int J Surg. 2016 Aug;32:89-98. doi: 10.1016/j.ijsu.2016.06.043. Epub 2016 Jul 6. Int J Surg. 2016. PMID: 27370542
References
-
- Williams BA, Kentor ML, Vogt MT, Vogt WB, Coley KC, Williams JP, et al. Economics of nerve block pain management after anterior cruciate ligament reconstruction: potential hospital cost savings via associated postanesthesia care unit bypass and same-day discharge. Anesthesiology. 2004;100(3):697–706. 10.1097/00000542-200403000-00034. - PubMed
-
- Hall-Burton DM, Hudson ME, Grudziak JS, Cunningham S, Boretsky K, Boretsky KR. Regional anesthesia is cost-effective in preventing unanticipated hospital admission in pediatric patients having anterior cruciate ligament reconstruction. Region Anesth Pain M. 2016;41(4):527–31. 10.1097/AAP.0000000000000410. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
