

Volatile sedation in critically ill adults undergoing mechanical ventilation: a meta-analysis of randomized controlled trials
- PMID: 40474220
- PMCID: PMC12142876
- DOI: 10.1186/s13054-025-05467-8
Volatile sedation in critically ill adults undergoing mechanical ventilation: a meta-analysis of randomized controlled trials
Abstract
Background: Volatile sedation has been associated with lung-protective effects, attenuation of inflammatory responses, and reduced organ dysfunction in critically ill patients. However, whether these potential benefits may translate into improvements in clinically relevant outcomes remains unclear. The primary aim of this meta-analysis of randomized controlled trials (RCTs) was to test the hypothesis that volatile sedation, compared to intravenous sedation, would reduce mortality in critically ill adults receiving mechanical ventilation.
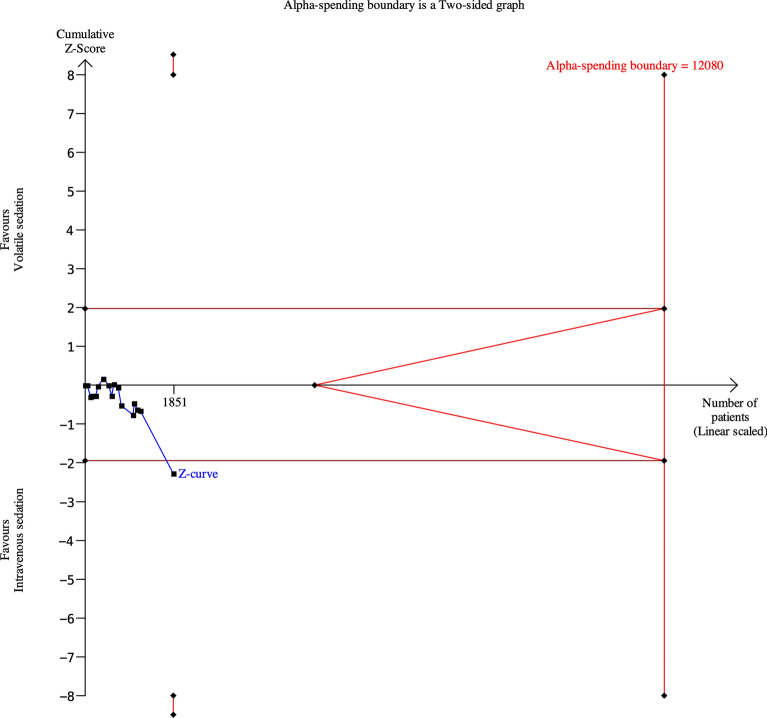
Methods: This study was registered in the PROSPERO database (CRD42023458064). We searched MEDLINE, Embase, and the Cochrane Library from inception until March 18, 2025, for RCTs comparing volatile sedatives with intravenous sedatives in critically ill patients undergoing invasive mechanical ventilation. The primary outcome was mortality at the longest follow-up. The secondary outcomes included duration of mechanical ventilation, length of hospital and intensive care unit (ICU) stay, hypotension, acute kidney injury, delirium, postoperative nausea and vomiting, atrial fibrillation, and time from sedative discontinuation to extubation. A random-effects Mantel-Haenszel meta-analysis was used for data synthesis. Trial sequential analysis (TSA) was performed to assess the robustness of the pooled data for the primary outcome.
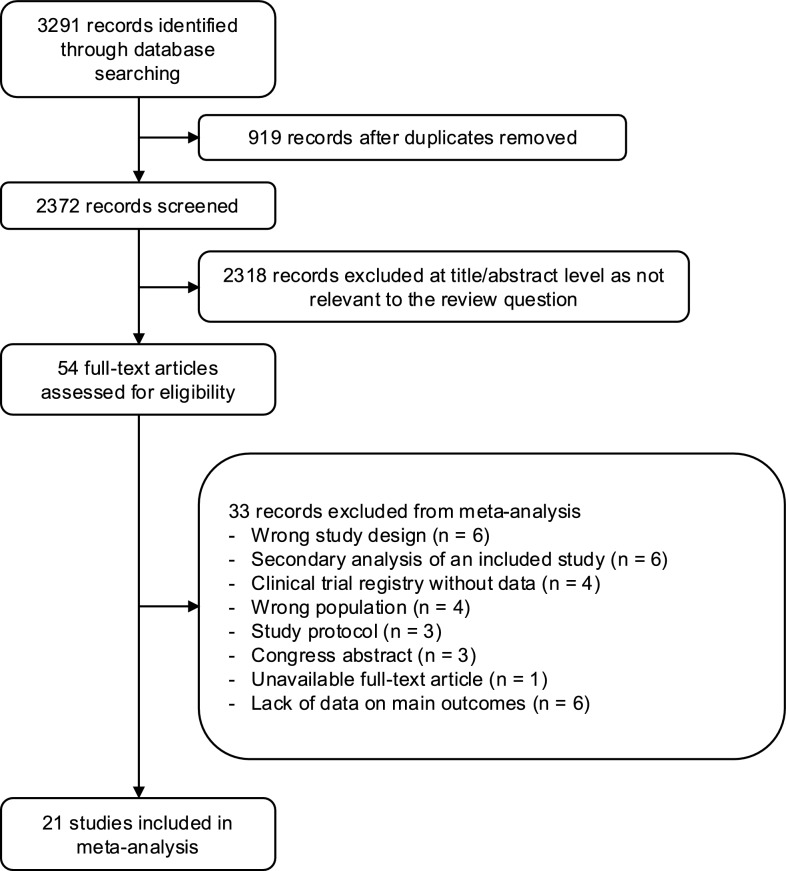
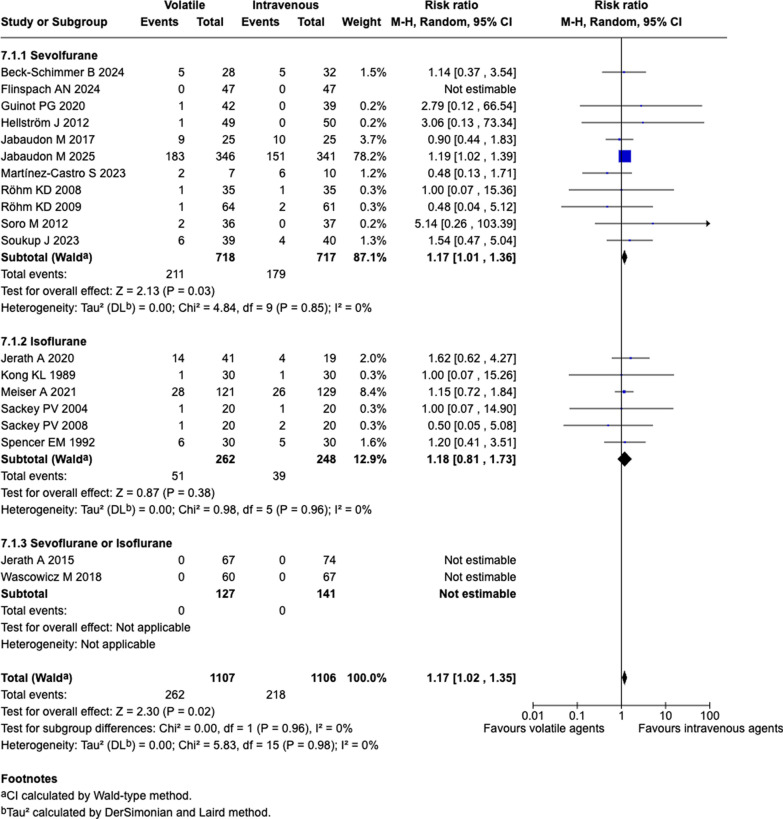
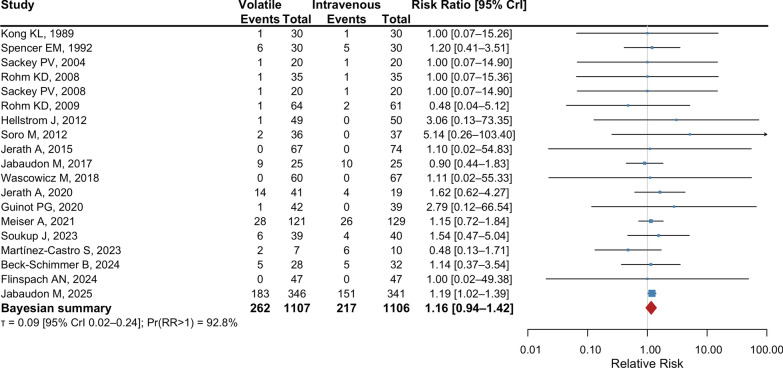
Results: We included 21 RCTs, comprising 2367 patients. Compared to intravenous sedation, volatile sedation may increase mortality at the longest follow-up (262/1107 vs. 218/1106; relative risk: 1.17; 95% confidence interval, 1.02 to 1.35; low certainty). However, TSA suggested a lack of definitive conclusion, as the required sample size was 12,080. No meaningful effects were observed on secondary outcomes, except for slightly shortened time from sedation termination to extubation (mean difference, - 90.62 min; 95% confidence interval, - 124.64 to - 56.60; low certainty), CONCLUSIONS: This meta-analysis of RCTs showed that, compared to intravenous sedation, volatile sedation may increase mortality among mechanically ventilated critically ill adults. Based on the current randomized evidence, its use in the ICU should be limited to carefully selected clinical scenarios. Further research is needed to identify patient populations that may benefit from this sedation strategy.
Keywords: Intensive care units; Mechanical ventilation; Meta-analysis; Sedation; Systematic review; Volatile anesthetics.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Comment in
-
Volatile agents: when generalization doesn't help.Crit Care. 2025 Jul 14;29(1):305. doi: 10.1186/s13054-025-05554-w. Crit Care. 2025. PMID: 40660349 Free PMC article. No abstract available.
-
Volatile sedation in critically ills adults undergoing mechanical ventilation: not all inhaled sedatives are equivalent!Crit Care. 2025 Aug 14;29(1):356. doi: 10.1186/s13054-025-05603-4. Crit Care. 2025. PMID: 40814053 Free PMC article. No abstract available.
-
Is volatile sedation truly associated with increased mortality in mechanically ventilated critically ill adults compared to intravenous sedation? Moving beyond pairwise meta-analysis to individual agent assessment via bayesian network meta-analysis.Crit Care. 2025 Oct 15;29(1):435. doi: 10.1186/s13054-025-05681-4. Crit Care. 2025. PMID: 41094679 Free PMC article. No abstract available.
References
-
- Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825. - PubMed
-
- Riker RR, Shehabi Y, Bokesch PM, Ceraso D, Wisemandle W, Koura F, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301:489–99. - PubMed
-
- Kotani Y, Pruna A, Landoni G. Mechanisms of action of the detrimental effects of propofol on survival. J Cardiothorac Vasc Anesth. 2023;37:2176–80. - PubMed
-
- FDA Drug Shortages [Internet]. [cited 2023 Nov 29]. Available from: https://www.accessdata.fda.gov/scripts/drugshortages/default.cfm
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
