

Monro-Kellie 4.0: moving from intracranial pressure to intracranial dynamics
- PMID: 40474297
- PMCID: PMC12142851
- DOI: 10.1186/s13054-025-05476-7
Monro-Kellie 4.0: moving from intracranial pressure to intracranial dynamics
Abstract
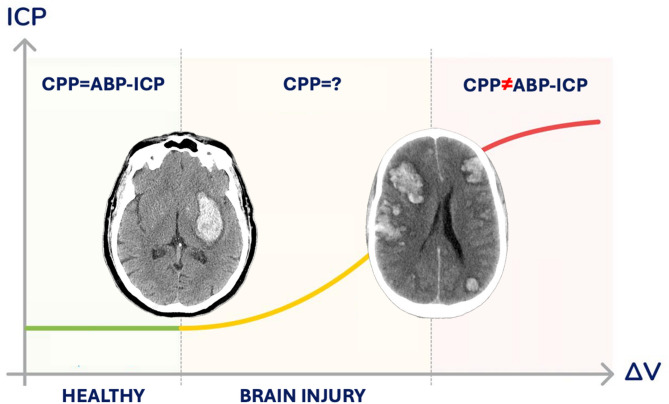
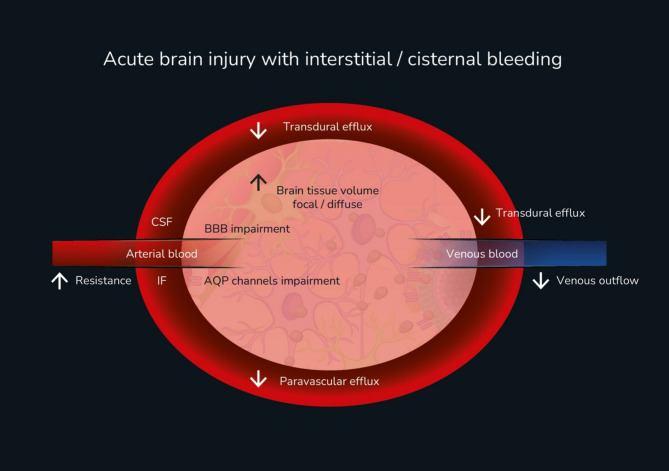
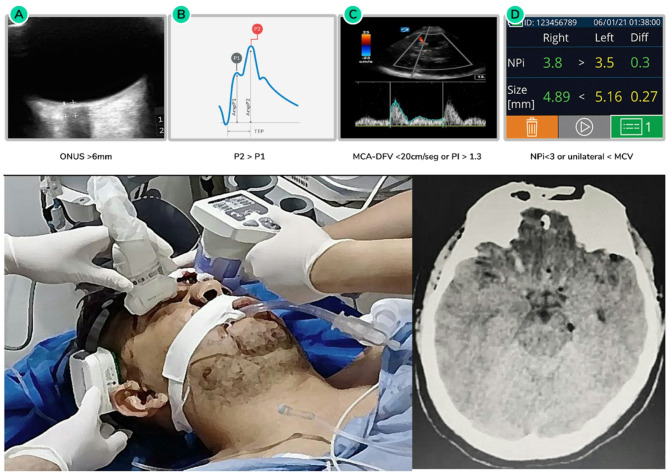
The Monro-Kellie doctrine, introduced in the late 18th century, was a groundbreaking concept aimed at explaining the interactions between intracranial volume components. It has since become a cornerstone of brain physiology, now recognized as intracranial dynamics. Initially, the doctrine focused on physiological observations of the three incompressible components of the cranial vault: brain tissue, blood, and cerebrospinal fluid (CSF). Over the centuries, advancements in neuroscience and medical technology have deepened our understanding of intracranial pressure (ICP) regulation, its pathophysiological implications and its role in neurological disorders. This revisitation of the Monro-Kellie doctrine examines how impairments in cerebrovascular autoregulation, brain compartmentalization and the glymphatic system interact in severely brain-injured patients, calling for new management strategies when facing these critical situations. Additionally, it reinforces the need for a holistic monitoring approach to improve early diagnostics and intervention. The evolution of ICP assessment has significantly shaped the management of brain trauma, spontaneous bleeding, ischemic stroke, and hydrocephalus. With the introduction of innovative tools such as brain ultrasound, automated pupillometry and noninvasive pressure waveform monitoring, ICP management is shifting toward more accessible and continuous evaluation strategies. This review explores how blending historical principles with cutting-edge innovations is transforming neuromonitoring and enhancing patient outcomes in critical care.
Keywords: Acute brain injury; Intracranial compartmental syndrome; Intracranial compliance; Intracranial pressure; Traumatic brain injury.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: Sérgio Brasil is a senior advisor for brain4care.
Figures

References
-
- Sonig A, Jumah F, Raju B, Patel NV, Gupta G, Nanda A. The historical evolution of intracranial pressure monitoring. World Neurosurg. 2020;138:491–7. - PubMed
-
- Lundberg N. The Saga of the Monro-Kellie doctrine. Berlin Heidelberg: Springer; 1983, pp. 68–76.
-
- Wu OC, Manjila S, Malakooti N, Cohen AR. The remarkable medical lineage of the Monro family: contributions of Alexander primus, secundus, and Tertius. J Neurosurg. 2012;116(6):1337–46. - PubMed
-
- Macintyre I. A hotbed of medical innovation: George Kellie (1770–1829), his colleagues at Leith and the Monro-Kellie doctrine. J Med Biogr. 2014;22(2):93–100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
