

The metabolic and autoregulatory profile of reversible delayed cerebral ischemia in unconscious patients after aneurysmal subarachnoid hemorrhage: a prospective multimodal neuromonitoring cohort study
- PMID: 40474300
- PMCID: PMC12142913
- DOI: 10.1186/s13054-025-05460-1
The metabolic and autoregulatory profile of reversible delayed cerebral ischemia in unconscious patients after aneurysmal subarachnoid hemorrhage: a prospective multimodal neuromonitoring cohort study
Abstract
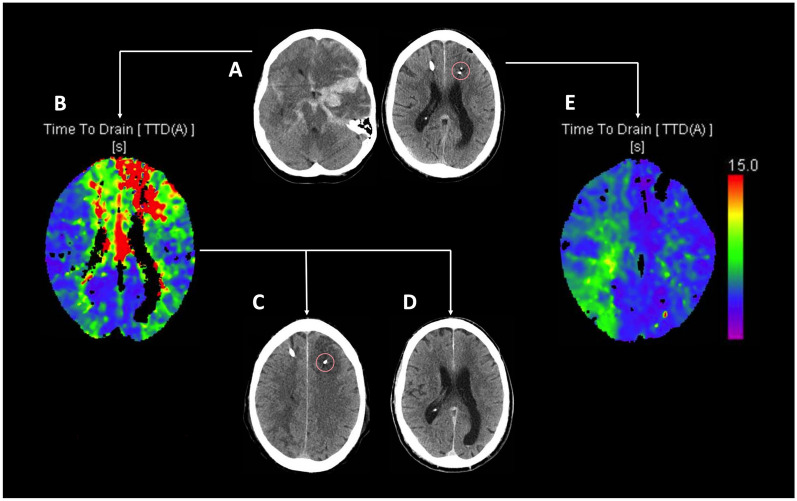
Background: The detection and treatment of delayed cerebral ischemia (DCI) following aneurysmal subarachnoid hemorrhage (SAH) remain challenging. Multimodal neuromonitoring and CT perfusion scanning (CTP) are promising tools for diagnosing DCI in unconscious patients. This study aims to compare the metabolic and autoregulatory characteristics of patients with cerebral hypoperfusion indicative of DCI that either resolves post-treatment or progresses to infarction due to treatment failure.
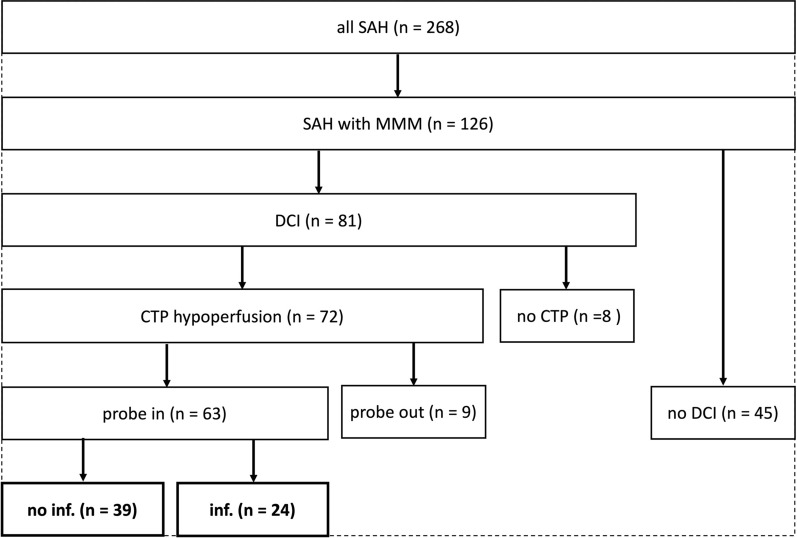
Methods: In a cohort of 268 consecutive SAH patients, neuromonitoring-comprising intracranial pressure (ICP) and brain tissue oxygen (PtiO2) measurements, and/or cerebral microdialysis-was implemented in 126 (47%) neurologically unassessable patients. Aberrant neuromonitoring measurements triggered CTP, and in cases of confirmed perfusion deficits, first-tier treatment involved induced hypertension. Non-responsive perfusion deficits were further evaluated with conventional angiography, and spasmolysis or angioplasty was performed if suitable vasospasm was identified. DCI-related infarction was noted on CT imaging at discharge, and clinical outcomes were assessed using the modified rankin scale (mRS) at 12 months. Using a generalized linear mixed-effects model (GLMM), factors associated with the occurrence of DCI-related infarction were assessed.
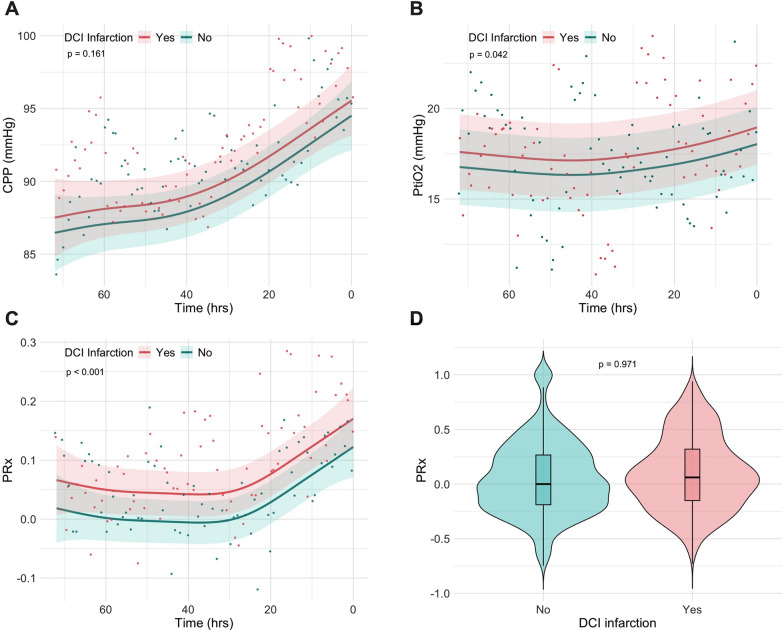
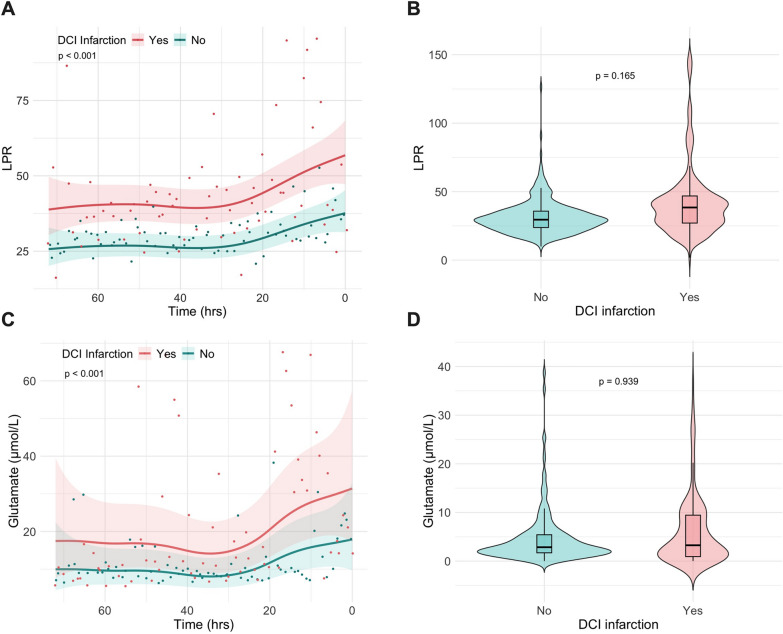
Results: CTP deficits were identified in 72 (57%) patients, of whom 63 (88%) had neuromonitoring probes near the affected areas. In 24 patients (38%), perfusion deficits progressed to infarction, while in 39 (62%), deficits were successfully reversed through induced hypertension or spasmolysis. In a GLMM, lower pressure reactivity index (PRx-OR 2.70, 95% CI 1.04-4.67; p < 0.001) and lower lactate-to-pyruvate ratio (LPR-OR 1.02, 95% CI 1.01-1.03; p < 0.001) were independently associated with better treatment response and reduced infarction risk, after adjusting for clinical hemorrhage severity. These effects were observed more than 24 h before cerebral hypoperfusion. Pooled PRx and LPR over this time frame were not associated with functional outcome.
Conclusion: Loss of cerebrovascular reactivity and metabolic disturbances precede cerebral hypoperfusion in SAH. Lower PRx and LPR levels are independently associated with improved DCI treatment efficacy. These findings must be interpreted in the context of study limitations, including the small sample size and the focal nature of microdialysis measurements. Nevertheless, the results suggest that invasive neuromonitoring may aid in identifying patients more likely to benefit from treatment.
Trial registration: This project was retrospectivly registered in the German Clinical Trial Register (DRKS00030505) on the third of January 2023.
Keywords: Cerebral autoregulation; Cerebral infarction; Cerebral microdialysis; Delayed cerebral ischemia; Perfusion computed tomography; Subarachnoid hemorrhage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to part: The trial was conducted in accordance with the recommendations of the ethics committee of the RWTH Aachen University Hospital. Informed consent was obtained from all included patients. Consent for publication: Not applicalbe. Competing interests: The authors declare no competing interests.
Figures
References
-
- Etminan N, Chang HS, Hackenberg K, de Rooij NK, Vergouwen MDI, Rinkel GJE, et al. Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region, time period, blood pressure, and smoking prevalence in the population: a systematic review and meta-analysis. JAMA Neurol. 2019;76(5):588–97. - DOI - PMC - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
