

Effectiveness of introducing pulse oximetry and clinical decision support algorithms for the management of sick children in primary care in Kenya and Senegal on referral and antibiotic prescription: the TIMCI quasi-experimental pre-post study
- PMID: 40474998
- PMCID: PMC12140026
- DOI: 10.1016/j.eclinm.2025.103196
Effectiveness of introducing pulse oximetry and clinical decision support algorithms for the management of sick children in primary care in Kenya and Senegal on referral and antibiotic prescription: the TIMCI quasi-experimental pre-post study
Abstract
Background: Acute illnesses are leading causes of death among children under-five, who often receive antibiotics unnecessarily, contributing to antimicrobial resistance. Pulse oximetry and digital Clinical Decision Support Algorithms (CDSAs) can strengthen the detection and management of severe childhood illnesses, and support antibiotic stewardship in primary care, but lack evidence for scale-up. This study sought to understand the real-world impact of these tools on urgent referrals and antibiotic prescription for children under-five.
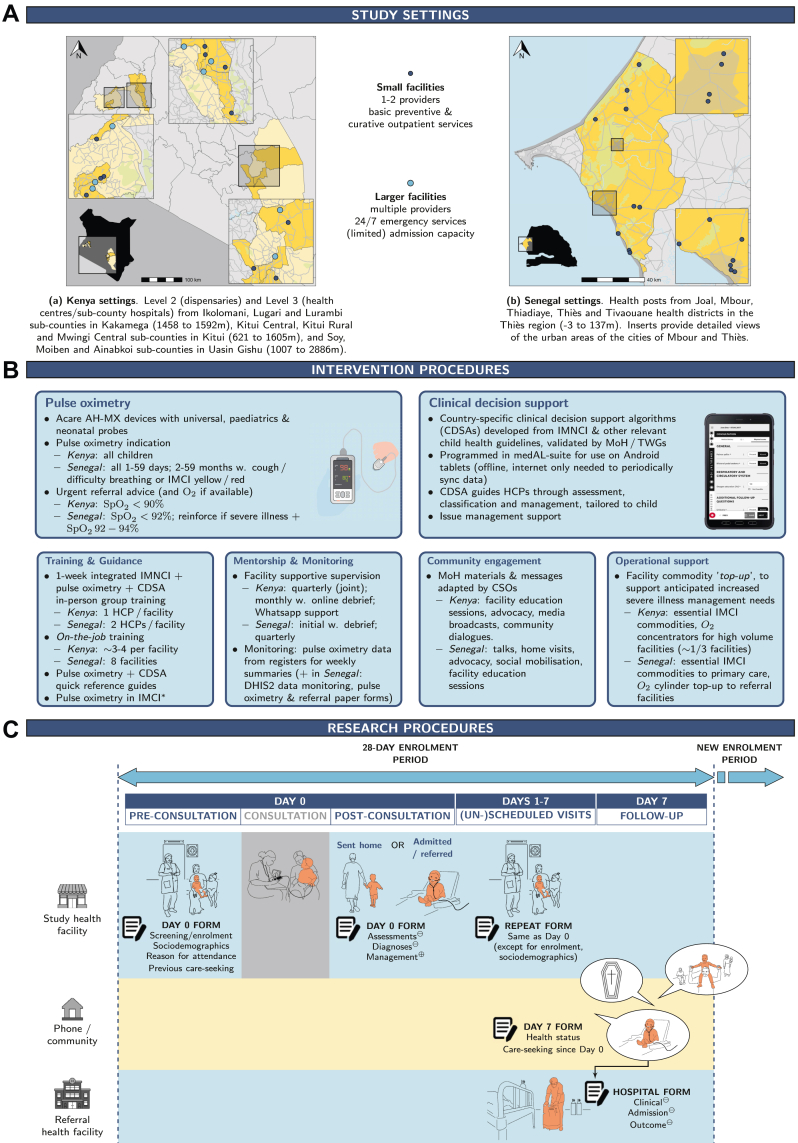
Methods: A quasi-experimental pre-post study of the implementation of pulse oximetry and CDSAs for healthcare providers (HCPs) managing sick children at primary care level was conducted in Kenya and Senegal. Sick children 0-59 months attending study facilities were eligible. Trained research assistants collected data from caregivers and facility records on Day 0, with a follow-up phone call at Day 7. Providers were advised to use pulse oximetry for all sick children in Kenya, and in Senegal for all 1-59 days, and for 2-59 months with cough or difficulty breathing, or a moderate to severe illness. Urgent referral was recommended for SpO2 <90% in Kenya and SpO2 <92% in Senegal. Primary outcomes were antibiotic prescription and urgent referral rates at Day 0. They were assessed using generalised estimating equations for logistic regression. Results were estimated in terms of odds ratios and risk differences (RDs), adjusted where computable. The study is registered with clinicaltrials.gov (NCT05065320).
Findings: A total of 50,580 sick children (1-59 days: 979 pre, 1748 post; 2-59 months: 16,782 pre, 31,071 post) were enrolled from September 13, 2021 to February 8, 2023 in Kenya and August 16, 2021 to March 31, 2023 in Senegal. In the pre-intervention period, urgent referrals were rare (0.6% in 1-59 days; 0.4% in 2-59 months), while antibiotic prescriptions were common (53.9% in 1-59 days; 74.9% in 2-59 months). Intervention uptake was 75% in Kenya and 40% in Senegal where a protracted HCP strike affected the intervention. The prevalence of SpO2 values prompting an urgent referral recommendation was 1.3% in 1-59 days and 0.8% in 2-59 months, but few of them resulted in actual referrals (26.1% in 1-59 days; 11.4% in 2-59 months). There was no change in overall urgent referrals (RD 0.2% [-0.5%, 0.9%] in 1-59 days; adjusted RD 0.2% [-0.2%, 0.5%] in 2-59 months). Antibiotic prescription rate was reduced by 14.6% [8.7%, 20.6%] in 1-59 days and by 22.6% [18.3%, 26.9%] in 2-59 months in the post-intervention period while caregiver-reported recovery rates at Day 7 remained stable.
Interpretation: When implemented in routine health systems at primary care level in Kenya and Senegal, pulse oximetry and CDSAs were not found to be associated with an increase in urgent referrals but likely mediated antibiotic prescription reductions. The absence of referral increase may stem from limited severe illness detection due to low hypoxaemia prevalence and barriers to referral, also affected in Senegal by a protracted post-intervention HCP strike. Strengthening the referral system and implementing broader antibiotic stewardship strategies are likely to be needed to improve the effectiveness of the intervention and its impact on child health outcomes.
Funding: Unitaid grant n°2019-35-TIMCI: Tools for Integrated Management of Childhood Illness.
Keywords: Child health; Clinical decision support; Hypoxaemia; Integrated management of childhood illness; Primary care; Pulse oximetry; Quasi-experimental study.
© 2025 The Authors.
Conflict of interest statement
The authors declare no competing interests. All institutes received funding as part of grant n°2019-35-TIMCI, contributing to salaries of co-authors.
Figures


References
-
- Fink G., D’Acremont V., Leslie H.H., Cohen J. Antibiotic exposure among children younger than 5 years in low-income and middle-income countries: a cross-sectional study of nationally representative facility-based and household-based surveys. Lancet Infect Dis. 2020;20:179–187. - PubMed
-
- Levine G.A., Bielicki J., Fink G. Cumulative antibiotic exposure in the first 5 Years of life: estimates for 45 low- and middle-income countries from demographic and health survey data. Clin Infect Dis. 2022;75:1537–1547. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
