

Extracorporeal membrane oxygenation bridge to transplant in the era of the lung composite allocation score
- PMID: 40475035
- PMCID: PMC12140043
- DOI: 10.1016/j.jhlto.2025.100273
Extracorporeal membrane oxygenation bridge to transplant in the era of the lung composite allocation score
Abstract
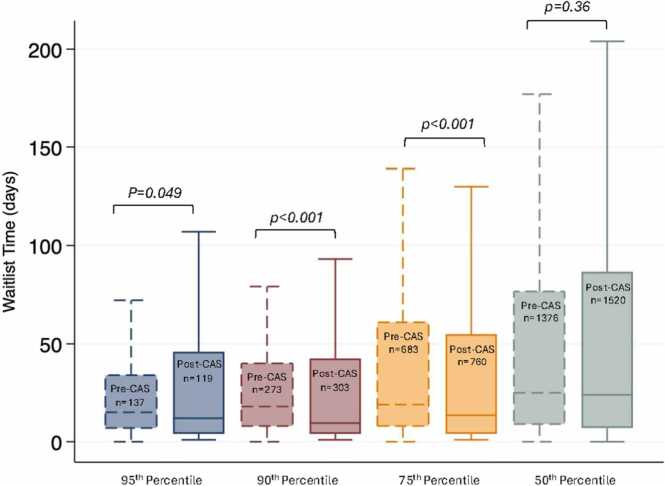
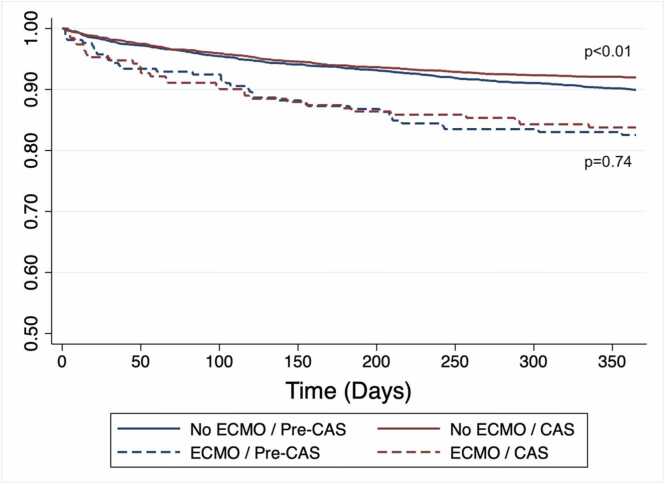
The lung composite allocation score (CAS) aims to improve waitlist outcomes for lung transplant candidates by prioritizing characteristics that reflect transplant urgency, including extracorporeal membrane oxygenation bridge to lung transplant (ECMO-BTT). Whether ECMO-BTT has been impacted by CAS is unknown. We analyzed the Organ Procurement and Transplant Network database to examine differences in ECMO-BTT utilization and characteristics and outcomes between transplant recipients who were transplanted one year before and one year after CAS implementation. Lung transplant recipients who received ECMO-BTT in the post-CAS era were younger (p < 0.01), more likely to be on ECMO at transplant listing rather than be initiated after (p < 0.05), and had shorter waitlist time (p < 0.01). Waitlist time was shorter in the post-CAS era among recipients (even non-ECMO) with high allocation scores only. This may have contributed to decreased use of ECMO-BTT in the post-CAS era (p = 0.03). One-year post-transplant survival did not differ between eras for ECMO-BTT patients, though was significantly better in the CAS era for non-ECMO-BTT patients (92% vs 90%, p < 0.01). We report initial results of ECMO-BTT utilization in the post-CAS era.
Keywords: Bridge-to-transplant; Composite allocation score; Extracorporeal membrane oxygenation; Lung transplantation; Waitlist time.
© 2025 International Society for Heart and Lung Transplantation.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Three-year outcomes after bridge to transplantation ECMO-pre- and post-2018 UNOS revised heart allocation system.J Heart Lung Transplant. 2024 Nov;43(11):1838-1845. doi: 10.1016/j.healun.2024.07.025. Epub 2024 Aug 7. J Heart Lung Transplant. 2024. PMID: 39122220
-
Extracorporeal membrane oxygenation as a bridge to advanced heart failure therapies.J Heart Lung Transplant. 2023 Aug;42(8):1059-1071. doi: 10.1016/j.healun.2023.02.1498. Epub 2023 Mar 1. J Heart Lung Transplant. 2023. PMID: 36964083
-
Outcomes of Recipients Aged 65 Years and Older Bridged to Lung Transplant With Extracorporeal Membrane Oxygenation.ASAIO J. 2024 Mar 1;70(3):230-238. doi: 10.1097/MAT.0000000000002092. Epub 2023 Nov 8. ASAIO J. 2024. PMID: 37939695 Free PMC article.
-
Extracorporeal membrane oxygenation as a bridge vs. non-bridging for lung transplantation: A systematic review and meta-analysis.Clin Transplant. 2021 Jan;35(1):e14157. doi: 10.1111/ctr.14157. Epub 2020 Dec 11. Clin Transplant. 2021. PMID: 33222260
-
Bridge to lung transplantation with extracorporeal membrane oxygenation support.Curr Opin Organ Transplant. 2012 Oct;17(5):496-502. doi: 10.1097/MOT.0b013e328357fa4f. Curr Opin Organ Transplant. 2012. PMID: 22941324 Review.
References
-
- Klapper J.A., Denlinger C., Hartwig M.G., Chang S.H. Discussions in cardiothoracic treatment and care: implications for the composite allocation score system for organ distribution in the United States. Semin Thorac Cardiovasc Surg. 2024;36:450–456. doi: 10.1053/j.semtcvs.2024.08.002. - DOI - PubMed
LinkOut - more resources
Full Text Sources
