

South Asians and cardiometabolic health: A framework for comprehensive care for the individual, community, and population - An American society for preventive cardiology clinical practice statement
- PMID: 40475260
- PMCID: PMC12139456
- DOI: 10.1016/j.ajpc.2025.101000
South Asians and cardiometabolic health: A framework for comprehensive care for the individual, community, and population - An American society for preventive cardiology clinical practice statement
Abstract
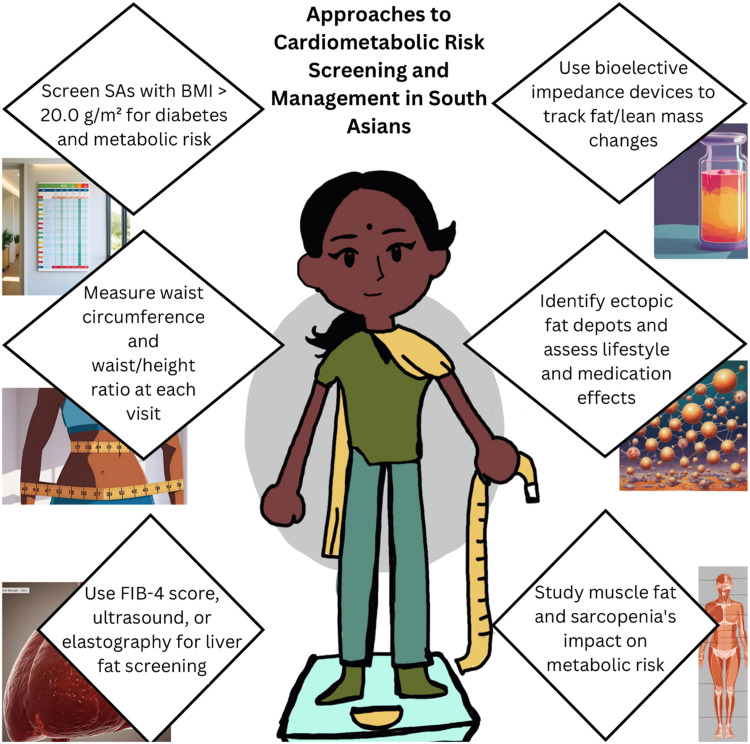
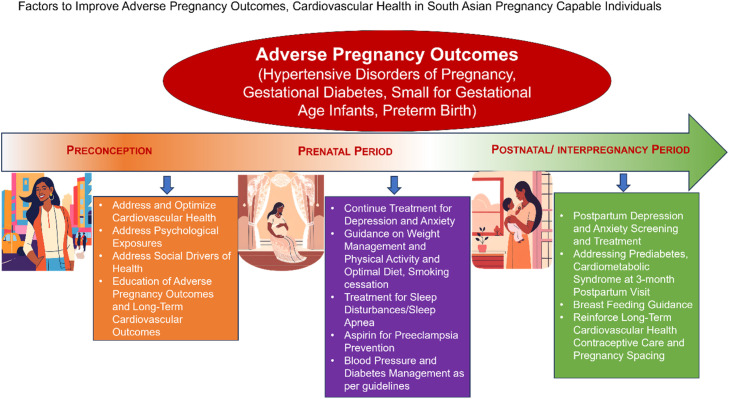
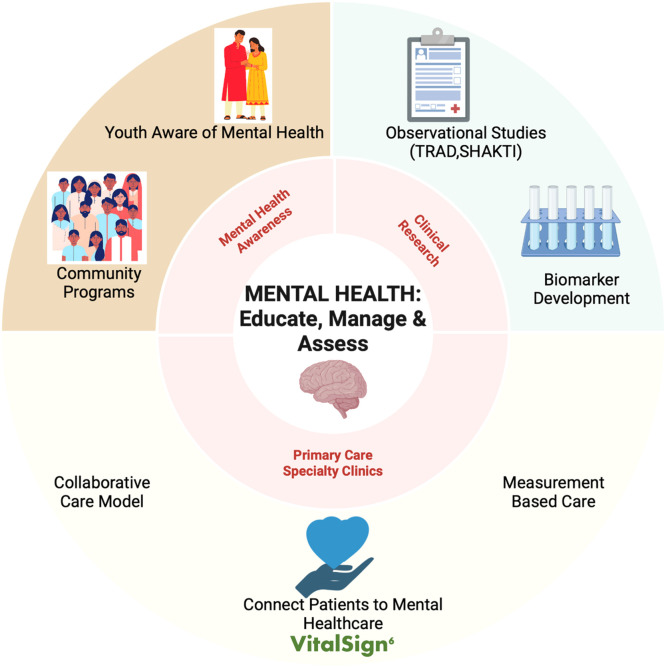
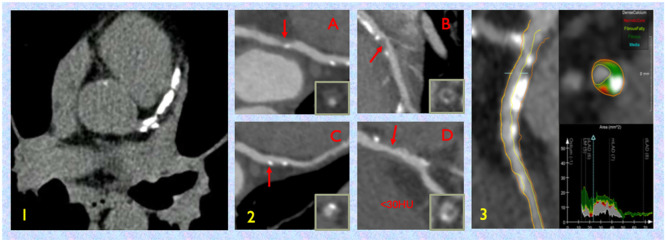
South Asians (SAs) represent an increasing proportion of North American populations and demonstrate excess cardiometabolic risk. Multiple factors likely contribute; however, much is not yet known about what leads to this excess risk. Diet composition, physical activity, and mental health are important lifestyle contributors. Specific adverse pregnancy outcomes are higher in SA women and represent an early opportunity for intervention. More broadly, comprehensive assessments of adiposity, diabetes, hypertension, dyslipidemia, coronary atherosclerosis via imaging, and genetic risk may improve detection and awareness among SAs and those treating SAs. At an individual level, culturally tailored preventive clinics may foster awareness and detection, leading to improved prevention and management of cardiometabolic risk. At a community and population level, assessments of the impact of social determinants, acculturation, and the environment may lead to broader initiatives to improve health in SAs. Lastly, supporting expanded investigation, policy, and other health and science measures at an institutional and societal level may lead to broad but impactful changes across the North American diaspora. In this clinical practice statement, we aim to provide a roadmap of the path forward in each of these domains for health care providers and health systems, community outreach groups, and stakeholders invested in investigation and policy to mitigate risk and empower SAs to lead healthy lives.
Keywords: Cardiometabolic; Coronary; Diabetes; Ethnic; Lifestyle; Prevention; Social determinants of health; South Asian.
© 2025 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Anand Rohatgi reports a relationship with Johnson & Johnson Services Inc that includes: speaking and lecture fees. Anand Rohatgi reports a relationship with Raydel Australia Pty Ltd that includes: consulting or advisory. Anand Rohatgi reports a relationship with CSL Behring LLC that includes: funding grants. Anand Rohatgi reports a relationship with Quest Diagnostics Inc that includes: non-financial support. Anand Rohatgi reports a relationship with SANSAR that includes: consulting or advisory. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Implications of the 2019 American College of Cardiology/American Heart Association Primary Prevention Guidelines and potential value of the coronary artery calcium score among South Asians in the US: The Mediators of Atherosclerosis in South Asians Living in America (MASALA) study.Atherosclerosis. 2021 Oct;334:48-56. doi: 10.1016/j.atherosclerosis.2021.08.030. Epub 2021 Aug 23. Atherosclerosis. 2021. PMID: 34481175 Free PMC article.
-
The social determinants of health associated with cardiometabolic diseases among Asian American subgroups: a systematic review.BMC Health Serv Res. 2022 Feb 25;22(1):257. doi: 10.1186/s12913-022-07646-7. BMC Health Serv Res. 2022. PMID: 35216607 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Profiles of cardiometabolic risk and acculturation indicators among South Asians in the US: latent class analysis of the MASALA study.Front Public Health. 2024 Oct 8;12:1384607. doi: 10.3389/fpubh.2024.1384607. eCollection 2024. Front Public Health. 2024. PMID: 39440183 Free PMC article.
References
LinkOut - more resources
Full Text Sources
