

Analysis of the International, Regional, and National Endocarditis-Related Disease Burdens (1990-2021), and Changes to Projections for the Next 15 Years: A Population-Based Study
- PMID: 40475722
- PMCID: PMC12135659
- DOI: 10.31083/RCM27168
Analysis of the International, Regional, and National Endocarditis-Related Disease Burdens (1990-2021), and Changes to Projections for the Next 15 Years: A Population-Based Study
Abstract
Background: Endocarditis can lead to health loss and even death, making it one of the major contributors to the global disease burden, with its incidence continuously increasing. This study aimed to assess the trends and frontier analysis of the worldwide burden of endocarditis over the past 30 years and to improve the predictions of its future burden by 2035.
Methods: We analyzed the trends of global endocarditis incidence, prevalence, deaths, and disability-adjusted life years (DALYs) at international, regional, and national levels from 1990 to 2021 using a comprehensive, localized, and multidimensional approach. Clustering analysis assessed the changing patterns of disease burden related to endocarditis in the Global Burden of Disease (GBD) study regions. Correlation analysis was conducted to determine the potential relationships between the burden of endocarditis and the socio-demographic index (SDI) and the Human Development Index (HDI). Frontier analysis was performed to identify possible areas for improvement and the disparities in development status among countries. Additionally, we projected the changes in the burden of endocarditis by 2035.
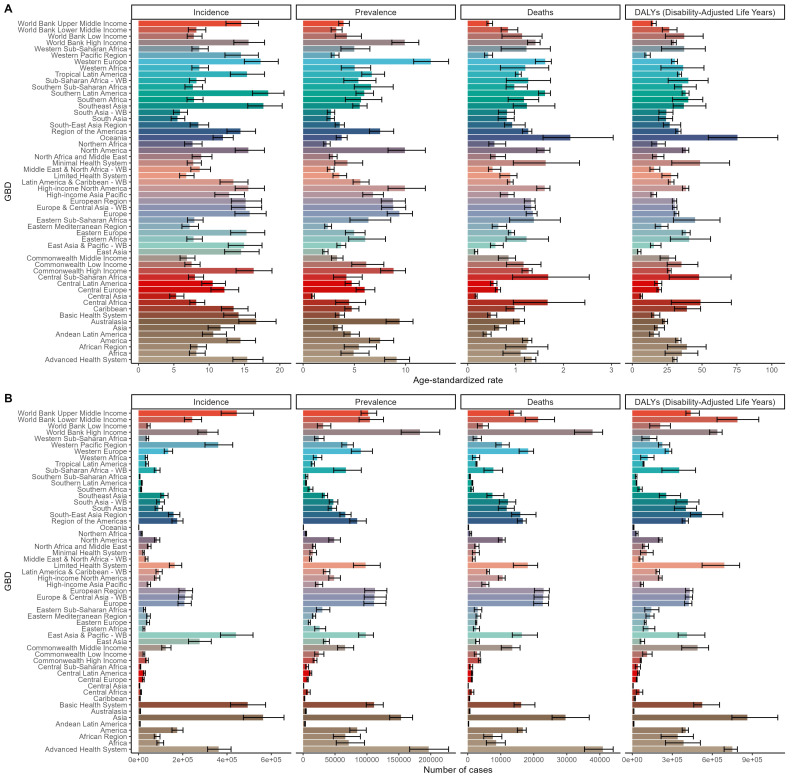
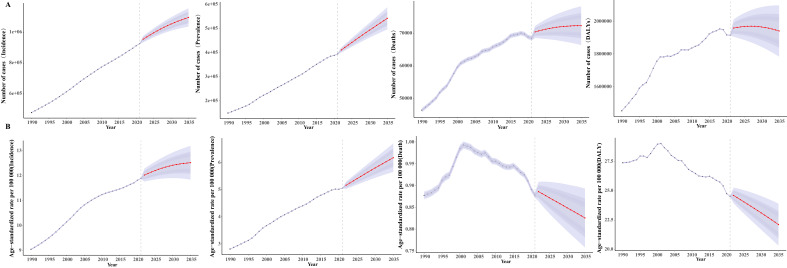
Results: From a global perspective, between 1990 and 2021, the incidence, prevalence, mortality, and DALYs associated with endocarditis have shown a continuous upward trend. At the national level, significant differences were observed in the incidence, prevalence, mortality, and DALYs of endocarditis worldwide. The United States had the highest number of deaths; India had the highest number of DALYs; Thailand had the highest incidence; Sri Lanka had the highest prevalence. The age-standardized rates (ASRs) for endocarditis prevalence, incidence, mortality, and DALYs increased steadily with age, peaking in the 95-year-old and above age group. The incidence, prevalence, mortality, and DALYs for males were 1.27 times, 1.02 times, 1.06 times, and 1.37 times those of females, respectively. Clustering analysis results indicated a significant increase in the estimated annual percentage change (EAPC) of mortality and DALY rates for endocarditis in East Asia. A significant correlation exists between EAPC and the ASRs of disease burden. Frontier analysis showed that countries and regions with higher SDIs have greater potential for improving the disease burden. The Bayesian age-period-cohort (BAPC) results indicated that the incidence, prevalence, mortality, and DALYs case numbers are expected to increase, with the ASRs for incidence and prevalence also projected to show a continuous upward trend by 2035.
Conclusions: The global burden of endocarditis, a significant public health issue, has shown an overall upward trend from 1990 to 2021. The continuous increase in the prevalence and incidence of endocarditis, driven by population growth and aging, has become a major challenge for its control and management, which may guide better public health policy formulation and the rational allocation of medical resources. This targeted approach is crucial for effectively alleviating the burden of this disease.
Keywords: GBD; deaths; disability-adjusted life-years; disease burden; endocarditis; incidence; prevalence.
Copyright: © 2025 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous
