

Healthcare responding to violence and abuse in Brazil: a quasi-experimental difference-in-differences analysis
- PMID: 40476048
- PMCID: PMC12135433
- DOI: 10.1016/j.lana.2025.101114
Healthcare responding to violence and abuse in Brazil: a quasi-experimental difference-in-differences analysis
Abstract
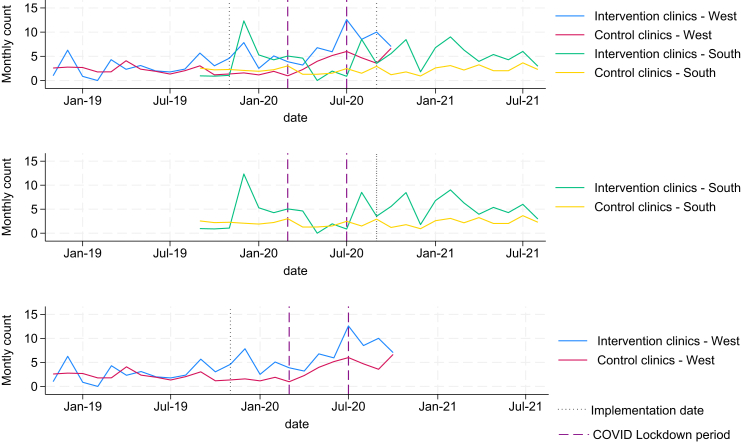
Background: Domestic violence against women (DVAW) is a public health issue and a breach of human rights, yet evidence on effective interventions remains limited, particularly in low-income and middle-income countries. This study aimed to evaluate changes in identification and referral to specialist support associated with system-level strategies implemented within Brazilian primary healthcare (PHC) to strengthen the response to DVAW. The strategies comprised an intervention called Healthcare Responding to Violence and Abuse (HERA).
Methods: Using a quasi-experimental design, HERA was implemented in eight PHC clinics, while 33 served as controls. Data on DVAW identification and referral were obtained from the national Epidemiological Surveillance System. Difference-in-differences analysis, using negative binomial regression, assessed HERA's impact, controlling for patient inflow, clinical supervision, COVID-19 lockdown, region, and clinic. Results are reported as marginal effects with 95% confidence intervals (CI).
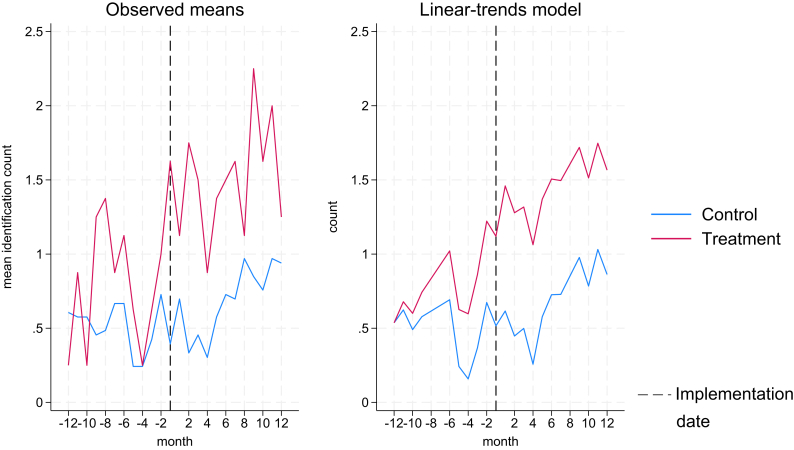
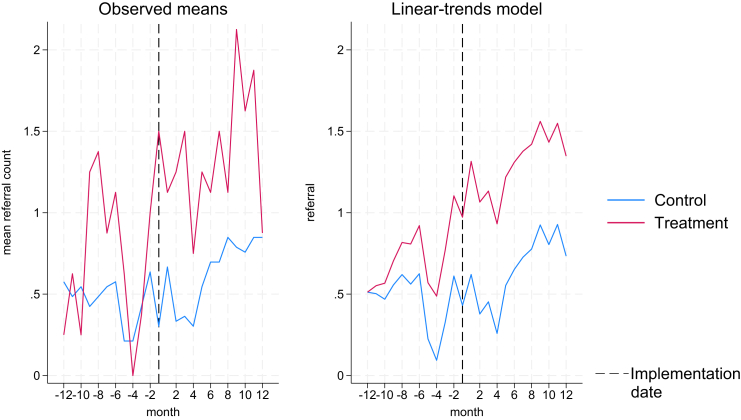
Findings: There was an increase in the probability of DVAW identification (0.47; 95% CI 0.18-0.77) and referral to support services (0.38; 95% CI 0.03-0.73), when adjusting for panel effects and time. The results were even larger when further controlling for additional variables (0.82 for identification [95% CI 0.44-1.21] and 0.87 for referrals [95% CI 0.47-1.29]).
Interpretation: HERA strategies increased DVAW identification and referral in PHC settings. Clinics implementing HERA were already more likely to identify and refer cases before the implementation, suggesting that HERA's strategies may be more effective in clinics that find DVAW interventions more acceptable, at least in Brazil.
Funding: NIHR Global Health Research Group Award.
Keywords: Domestic violence; Intervention; Low and middle income countries; Primary healthcare; Violence against women.
© 2025 The Author(s).
Conflict of interest statement
Estela Capelas Barbosa and Gene Feder reports salary support from the UK Prevention Research Partnership (Violence, Health and Society; MR-VO49879/1) for the present manuscript. This partnership is funded by the British Heart Foundation, Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Health and Social Care Research and Development Division (Welsh Government), Medical Research Council, National Institute for Health and Care Research, Natural Environment Research Council, Public Health Agency (Northern Ireland), The Health Foundation, and Wellcome. Gene Feder reports honoraria for clinician teaching events and institutional support from the NIHR for the present manuscript. He also declares travel support from the Global Burden of Disease programme and serves as an unpaid trustee for IRISi. All other authors declare no competing interests.
Figures
Similar articles
-
An evidence-based primary health care intervention to address domestic violence against women in Brazil: a mixed method evaluation.BMC Prim Care. 2023 Sep 25;24(1):198. doi: 10.1186/s12875-023-02150-1. BMC Prim Care. 2023. PMID: 37749549 Free PMC article.
-
Evaluation of a domestic violence training and support intervention in Palestinian primary care clinics in the west bank: a mixed method study.BMC Prim Care. 2025 Apr 4;26(1):97. doi: 10.1186/s12875-025-02751-y. BMC Prim Care. 2025. PMID: 40186105 Free PMC article.
-
Adaptive work in the primary health care response to domestic violence in occupied Palestinian territory: a qualitative evaluation using Extended Normalisation Process Theory.BMC Fam Pract. 2021 Jan 2;22(1):3. doi: 10.1186/s12875-020-01338-z. BMC Fam Pract. 2021. PMID: 33388033 Free PMC article.
-
Effects of second responder programs on repeat incidents of family abuse: An updated systematic review and meta-analysis.Campbell Syst Rev. 2022 Jan 28;18(1):e1217. doi: 10.1002/cl2.1217. eCollection 2022 Mar. Campbell Syst Rev. 2022. PMID: 36913197 Free PMC article. Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
References
-
- World Health Assembly (49) Prevention of violence: public health priority. 1996. https://iris.who.int/bitstream/handle/10665/179463/WHA49_R25_eng.pdf?seq...
-
- World Health Organization (WHO) Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. 2013. https://iris.who.int/bitstream/handle/10665/85240/9789241548595_eng.pdf - PubMed
-
- Garcia-Moreno C., Jansen H.A., Ellsberg M., Heise L., Watts C.H. Prevalence of intimate partner violence: findings from the WHO multi-country study on women's health and domestic violence. Lancet. 2006;368(9543):1260–1269. - PubMed
LinkOut - more resources
Full Text Sources
