

Streptococcal Serology Reference Intervals in an Australian Pediatric Cohort
- PMID: 40476715
- PMCID: PMC12343097
- DOI: 10.1093/jpids/piaf054
Streptococcal Serology Reference Intervals in an Australian Pediatric Cohort
Abstract
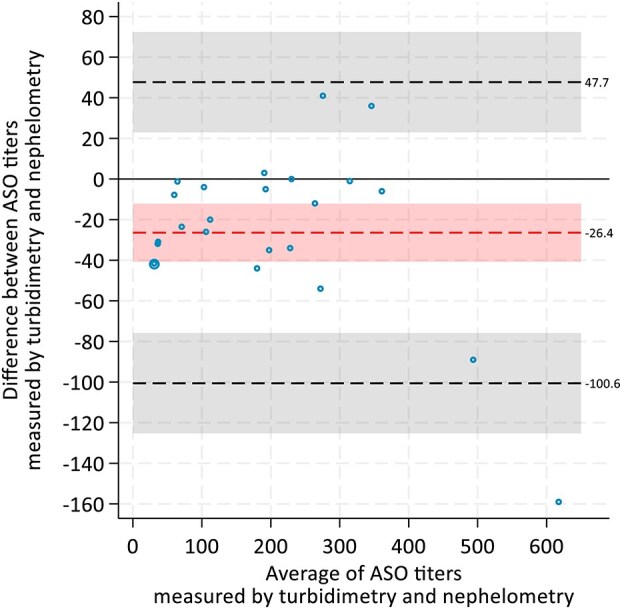
Background: Diagnostic criteria for acute rheumatic fever and post-streptococcal glomerulonephritis, the 2 major autoimmune complications of Streptococcus pyogenes infection, include serological evidence of preceding infection. The S. pyogenes proteins, namely streptolysin O and deoxyribonuclease B, are the most widely used targets for clinical streptococcal serology. We aimed to establish age-based reference intervals (RIs) for healthy children in Victoria, Australia, to guide interpretation of anti-streptolysin O (ASO) levels measured by turbidimetry and nephelometry, and anti-deoxyribonuclease B (ADB) levels by nephelometry.
Methods: Serum samples were collected from healthy pediatric cohorts aged 32-week gestation to <18 years at 4 hospitals in Melbourne, Australia, between February 2015 and October 2018. Anti-streptolysin O levels were measured in 2 cohorts: by turbidimetry in cohort 1 and by nephelometry in cohort 2. Anti-deoxyribonuclease B levels were measured by nephelometry in cohort 2. Reference intervals (RIs) for each age group were generated, including 80% upper limit of normal (ULN) cut-offs.
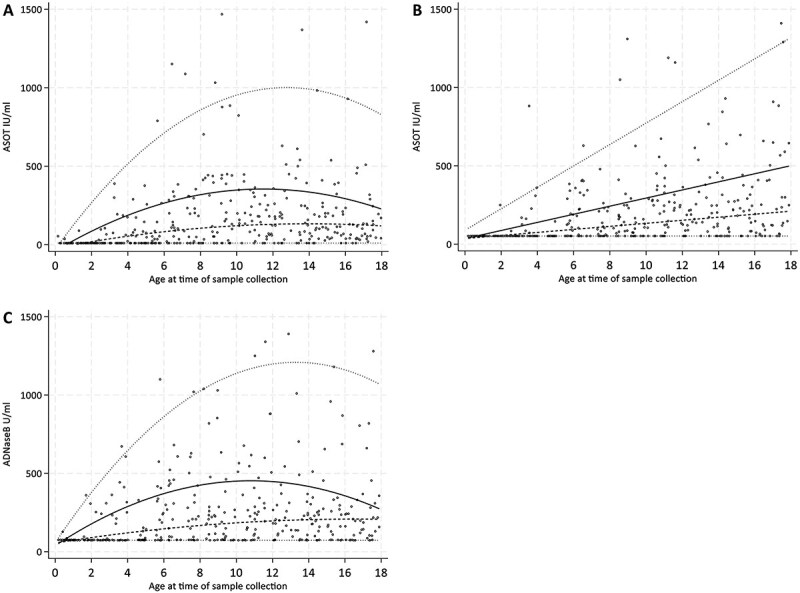
Results: Anti-streptolysin O levels were measured by turbidimetry for 359 samples from cohort 1, and ASO and ADB levels were measured by nephelometry for 360 samples from cohort 2. Anti-streptolysin O levels, measured by turbidimetry, were highest in children 5-9 years of age (80% ULN 346 IU/mL) in cohort 1. For cohort 2, there was a linear age-related increase in ASO levels measured by nephelometry (80% ULN 426 IU/mL in those 15 to <18 years old) and ADB levels were highest in children aged 10-14 years (80% ULN 454 IU/mL).
Conclusions: We established age-specific RI for ASO and ADB levels measured by turbidimetry and nephelometry for healthy Australian children. This study highlights the importance of local method-specific age-based RI to interpret ASO and ADB levels when clinicians suspect acute rheumatic fever or post-streptococcal glomerulonephritis in children.
Keywords: Streptococcus pyogenes; antibodies; child; deoxyribonuclease B; streptolysin O.
Plain language summary
This study established age-specific reference intervals for anti-streptolysin O and anti-DNAse B levels measured by turbidimetry and nephelometry for healthy Australian children. The values are higher than in adults, adding to global data regarding pediatric streptococcal serology values.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Pediatric Infectious Diseases Society.
Conflict of interest statement
None declared.
Figures
References
-
- Taylor A, Morpeth S, Webb R, Taylor S. The utility of rapid group A Streptococcus molecular testing compared with throat culture for the diagnosis of group A streptococcal pharyngitis in a high-incidence rheumatic fever population. J Clin Microbiol. 2021;59:e0097821. 10.1128/JCM.00978-21 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
