

Prone position: how understanding and clinical application of a technique progress with time
- PMID: 40478142
- PMCID: PMC9995262
- DOI: 10.1007/s44254-022-00002-2
Prone position: how understanding and clinical application of a technique progress with time
Abstract
Historical background: The prone position was first proposed on theoretical background in 1974 (more advantageous distribution of mechanical ventilation). The first clinical report on 5 ARDS patients in 1976 showed remarkable improvement of oxygenation after pronation.
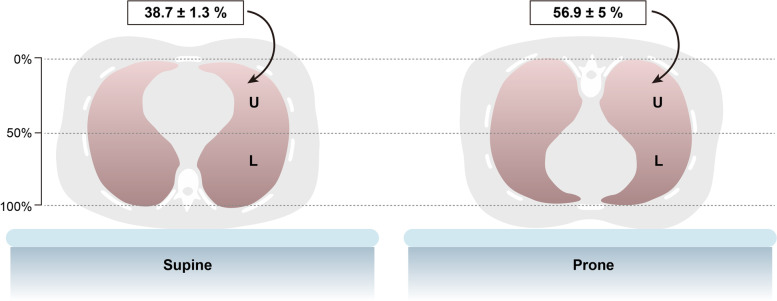
Pathophysiology: The findings in CT scans enhanced the use of prone position in ARDS patients. The main mechanism of the improved gas exchange seen in the prone position is nowadays attributed to a dorsal ventilatory recruitment, with a substantially unchanged distribution of perfusion. Regardless of the gas exchange, the primary effect of the prone position is a more homogenous distribution of ventilation, stress and strain, with similar size of pulmonary units in dorsal and ventral regions. In contrast, in the supine position the ventral regions are more expanded compared with the dorsal regions, which leads to greater ventral stress and strain, induced by mechanical ventilation.
Outcome in ards: The number of clinical studies paralleled the evolution of the pathophysiological understanding. The first two clinical trials in 2001 and 2004 were based on the hypothesis that better oxygenation would lead to a better survival and the studies were more focused on gas exchange than on lung mechanics. The equations better oxygenation = better survival was disproved by these and other larger trials (ARMA trial). However, the first studies provided signals that some survival advantages were possible in a more severe ARDS, where both oxygenation and lung mechanics were impaired. The PROSEVA trial finally showed the benefits of prone position on mortality supporting the thesis that the clinical advantages of prone position, instead of improved gas exchange, were mainly due to a less harmful mechanical ventilation and better distribution of stress and strain. In less severe ARDS, in spite of a better gas exchange, reduced mechanical stress and strain, and improved oxygenation, prone position was ineffective on outcome.
Prone position and covid-19: The mechanisms of oxygenation impairment in early COVID-19 are different than in typical ARDS and relate more on perfusion alteration than on alveolar consolidation/collapse, which are minimal in the early phase. Bronchial shunt may also contribute to the early COVID-19 hypoxemia. Therefore, in this phase, the oxygenation improvement in prone position is due to a better matching of local ventilation and perfusion, primarily caused by the perfusion component. Unfortunately, the conditions for improved outcomes, i.e. a better distribution of stress and strain, are almost absent in this phase of COVID-19 disease, as the lung parenchyma is nearly fully inflated. Due to some contradictory results, further studies are needed to better investigate the effect of prone position on outcome in COVID-19 patients.
Keywords: ARDS; Covid-19; Gas exchange; Lung mechanics; Prone position.
© The Author(s) 2023.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures






References
-
- Bryan AC. Conference on the scientific basis of respiratory therapy. Pulmonary physiotherapy in the pediatric age group. Comments of a devil’s advocate. Am Rev Respir Dis. 1974;110:143–4. - PubMed
-
- Douglas WW, Rehder K, Beynen FM, Sessler AD, Marsh HM. Improved oxygenation in patients with acute respiratory failure: the prone position. Am Rev Respir Dis. 1977;115:559–66. - PubMed
Publication types
LinkOut - more resources
Full Text Sources