

Clinical Significance of Somatic PIK3CA and MAP3K3 Mutations in Cerebral and Spinal Cavernous Malformations
- PMID: 40478424
- PMCID: PMC12596314
- DOI: 10.1007/s12975-025-01360-2
Clinical Significance of Somatic PIK3CA and MAP3K3 Mutations in Cerebral and Spinal Cavernous Malformations
Abstract
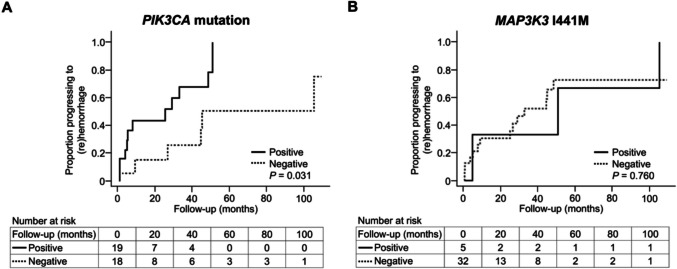
Somatic PIK3CA and MAP3K3 mutations in cerebral and spinal cavernous malformations (CMs) have been identified in recent studies. However, their significance in the clinical presentation and risk of hemorrhage in CMs remains poorly understood. We aimed to analyze the association between these mutations and the clinical characteristics of CMs. Among patients with CMs who underwent surgical resection of lesions between July 2002 and March 2022, those with complete clinical and radiological data at the time of initial surgery were included. Somatic PIK3CA and MAP3K3 mutations were detected using droplet digital polymerase chain reaction. Subsequently, the clinical and radiological characteristics correlated with these mutations were assessed. Furthermore, the effect of these mutations on the first symptomatic intraparenchymal hemorrhage during follow-up was evaluated. In total, 72 patients were included; among them, 50 had sufficient mutation data. PIK3CA E542K, E545K, and H1047R mutations were identified in 7 (14%), 7 (14%), and 15 (30%) patients, respectively. MAP3K3 I441M was identified in 10 (20%) patients (8 [16%] had both PIK3CA and MAP3K3 mutations). MAP3K3 I441M was more common in patients with Zabramski classification type II lesions than in those with CMs of other types (p = 0.024). Multivariate Cox regression analyses identified the presence of a PIK3CA mutation as a risk factor for early (re)hemorrhage. The results suggest that PIK3CA and MAP3K3 mutations are associated with clinical and radiological characteristics in patients with CMs and that the presence of a somatic PIK3CA mutation increases susceptibility to hemorrhage. These findings may help guide future therapeutic strategies.
Keywords: MAP3K3; PIK3CA; Cavernous malformations; Hemorrhage; Somatic mutations.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics Approval: This study was conducted in accordance with the Declaration of Helsinki and was approved by the Human Genome, Gene Analysis Research Ethics Committee of the Faculty of Medicine, The University of Tokyo (G10026, G10028, 2019211G), Ethics Committee of Tokyo Metropolitan Neurological Hospital (TS-R02-003), Ethics Committee of Fuji Brain Institute and Hospital (202103), and the Ethics Committee of Kanto Neurosurgical Hospital (2021–016). Consent to Participate: Written informed consent was obtained from each patient for inclusion in this study. Consent to Publish: Not applicable. Competing Interests: The authors declare no competing interests.
Figures

References
-
- Hong T, Xiao X, Ren J, et al. Somatic MAP3K3 and PIK3CA mutations in sporadic cerebral and spinal cord cavernous malformations. Brain. 2021;144:2648–58. 10.1093/brain/awab117. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous