

Primary Care Physician Characteristics and Low-Value Care Provision in Japan
- PMID: 40478554
- PMCID: PMC12144622
- DOI: 10.1001/jamahealthforum.2025.1430
Primary Care Physician Characteristics and Low-Value Care Provision in Japan
Abstract
Importance: Evidence is limited regarding the physician characteristics associated with the provision of low-value services in primary care, especially outside of the US.
Objective: To measure physician-level use of 10 low-value care services that provide no net clinical benefit and to investigate the characteristics of primary care physicians who frequently provide low-value care in Japan.
Design, setting, and participants: This cross-sectional analysis used a nationwide electronic health record database linked with claims data in Japan to assess visits by adult patients (age ≥18 years) to a solo-practice primary care physician from October 1, 2022, through September 30, 2023. Data analysis was performed from June 2024 to February 2025.
Main outcomes and measures: Multivariable-adjusted composite rate of low-value care services delivered per 100 patients per year, aggregated across 10 low-value measures, after accounting for case mix and other characteristics.
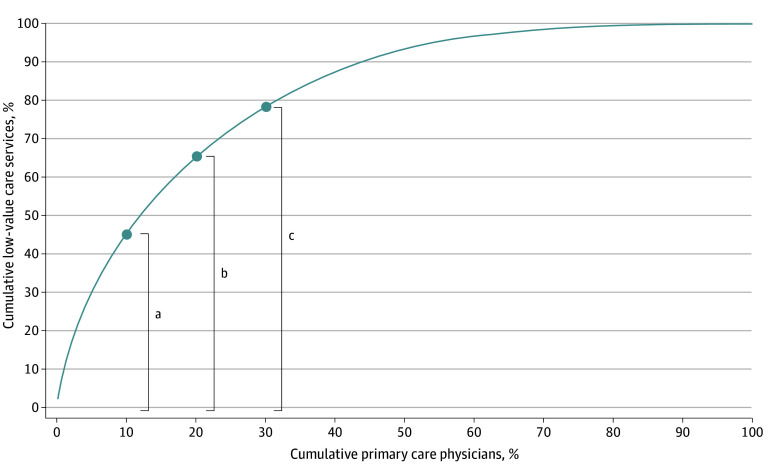
Results: Among 2 542 630 patients (mean [SD] age, 51.6 [19.8] years; 58.2% female) treated by 1019 primary care physicians (mean [SD] age 56.4 [10.2] years; 90.4% male), 436 317 low-value care services were identified (17.2 cases per 100 patients overall). Nearly half of these low-value care services were provided by 10% of physicians. After accounting for patient case mix, older physicians (age ≥60 years) delivered 2.1 per 100 patients (95% CI, 1.0-3.3) more low-value care services than those younger than 40 years; not board-certified physicians delivered 0.8 per 100 patients (95% CI, 0.2-1.5) more than general internal medicine board-certified physicians; physicians with higher patient volumes delivered 2.3 per 100 patients (95% CI, 1.5-3.2) more than those with low patient volumes; and physicians practicing in Western Japan delivered 1.0 per 100 patients (95% CI, 0.5-1.5) more than those in Eastern Japan.
Conclusions and relevance: The findings of this cross-sectional analysis suggest that low-value care services were common and concentrated among a small number of primary care physicians in Japan, with older physicians and not board-certified physicians being more likely to provide low-value care. Policy interventions targeting at a small number of certain types of physicians providing large quantities of low-value care may be more effective and efficient than those targeting all physicians uniformly.
Conflict of interest statement
Figures
References
-
- Brooks DJ, Reyes CE, Chien AT. Time to set aside the term ‘Low-Value Care’: focus on achieving high-value care for all. Health Affairs Forefront. https://www.healthaffairs.org/content/forefront/time-set-aside-term-low-...
MeSH terms
LinkOut - more resources
Full Text Sources
