

The TMA team and TTP pathway improved outcomes in a cohort with Thrombotic thrombocytopenic purpura
- PMID: 40478853
- PMCID: PMC12143514
- DOI: 10.1371/journal.pone.0325417
The TMA team and TTP pathway improved outcomes in a cohort with Thrombotic thrombocytopenic purpura
Abstract
Background: Providing optimal care for patients with thrombotic thrombocytopenic purpura (TTP) is challenging because of multiple involved specialties, knowledge gaps, and a high rate of disease relapse. A thrombotic microangiopathy (TMA) Team and TTP Pathway could improve outcomes.
Objectives: To assess if a structured TTP Pathway, supported by a TMA Team, improved TTP care by reducing TTP relapse and TTP-related death (TTP-RRD) at a rural Appalachian medical center.
Methods: Prospective cohort quality improvement project using the DMAIC quality improvement framework (Define, Measure, Analyze, Improve, Control) to develop a TMA Team and TTP Pathway. Pathway care included standardized use of therapeutic plasma exchange (TPE), rituximab, caplacizumab, as well as improved coordination between medical services, and regular outpatient biochemical TTP surveillance. Outcomes were determined by retrospective chart review for patients with acute TTP treated with usual care (N = 16 episodes) and the TTP Pathway (N = 16 episodes).
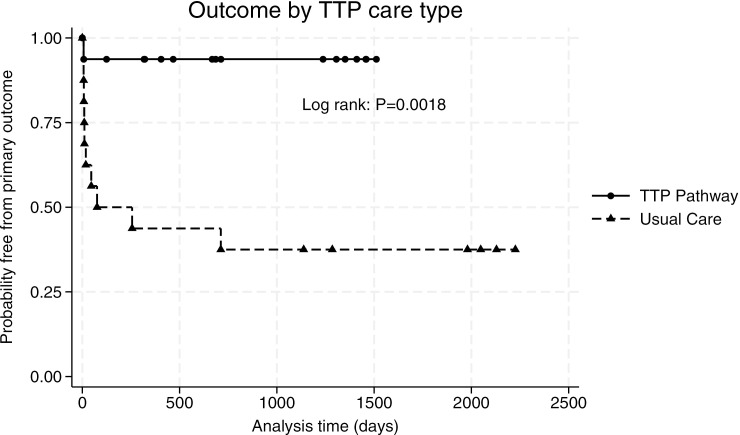
Results and conclusions: All patients had acquired TTP. TTP-RRD at 90 days was reduced from 69% with usual care to 6% with Pathway care (95% CI 0.35 to 0.90, P = 0.0004), a relative risk reduction of 91%; TTP relapse alone at 90 days was reduced from 62% to 0% (95% CI 0.36 to 0.88, P = 0.0002) with Pathway care. The number needed to treat to prevent TTP-RRD was 1.59 at 90 days. Over the project duration usual care demonstrated a hazard ratio for TTP-RRD of 12.58 compared to Pathway care. With the intervention, the duration of TPE was increased (median 6 vs 12 sessions, P < 0.05), as was use of rituximab (31.3% vs 93.8%, 95% CI -0.36 to -0.88, P = 0.003), and caplacizumab (6.3% vs 62.5%, 95% CI -0.027 to -0.81, P = 0.001). All Pathway patients underwent biochemical surveillance, and 31% had pre-emptive rituximab to reduce possibility of clinical relapse. A structured TTP Pathway significantly reduces morbidity and aligns care with modern clinical guidelines. The TMA Team is a valuable institutional resource to improve outcomes.
Copyright: © 2025 Merrill et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
SAM reports previous consultancy for Genentech, Sanofi, and the American Society of Hematology. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Caplacizumab Treatment for Acquired Thrombotic Thrombocytopenic Purpura.N Engl J Med. 2019 Jan 24;380(4):335-346. doi: 10.1056/NEJMoa1806311. Epub 2019 Jan 9. N Engl J Med. 2019. PMID: 30625070 Clinical Trial.
-
Cost effectiveness of caplacizumab in acquired thrombotic thrombocytopenic purpura.Blood. 2021 Feb 18;137(7):969-976. doi: 10.1182/blood.2020006052. Blood. 2021. PMID: 33280030 Free PMC article.
-
A regimen with caplacizumab, immunosuppression, and plasma exchange prevents unfavorable outcomes in immune-mediated TTP.Blood. 2021 Feb 11;137(6):733-742. doi: 10.1182/blood.2020008021. Blood. 2021. PMID: 33150928 Free PMC article.
-
Refining the standard of care in immune thrombotic thrombocytopenic purpura.Clin Adv Hematol Oncol. 2024 Oct;22(8):381-391. Clin Adv Hematol Oncol. 2024. PMID: 39356816 Review.
-
Beyond plasma exchange: novel therapies for thrombotic thrombocytopenic purpura.Hematology Am Soc Hematol Educ Program. 2018 Nov 30;2018(1):539-547. doi: 10.1182/asheducation-2018.1.539. Hematology Am Soc Hematol Educ Program. 2018. PMID: 30504355 Free PMC article. Review.
References
-
- Connelly-Smith L, Alquist CR, Aqui NA, Hofmann JC, Klingel R, Onwuemene OA, et al.. Guidelines on the Use of Therapeutic Apheresis in Clinical Practice - Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Ninth Special Issue. J Clin Apher. 2023;38(2):77–278. doi: 10.1002/jca.22043 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
