

Proteogenomic analysis of the CALGB 40601 (Alliance) HER2+ breast cancer neoadjuvant trial reveals resistance biomarkers
- PMID: 40480221
- PMCID: PMC12208316
- DOI: 10.1016/j.xcrm.2025.102154
Proteogenomic analysis of the CALGB 40601 (Alliance) HER2+ breast cancer neoadjuvant trial reveals resistance biomarkers
Abstract
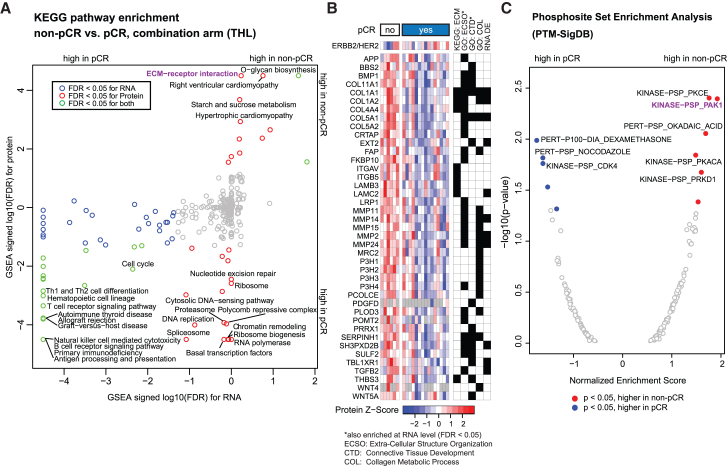
Proteogenomic analysis is applied to samples from the CALGB 40601 (Alliance) randomized neoadjuvant trial of trastuzumab, lapatinib, or the combination to identify biomarkers associated with pathological response status. Absence of ERBB2 gene amplification and human epidermal growth factor receptor 2 (HER2) protein overexpression by proteogenomics is associated with non-pathological compete response (pCR) (p < 0.05), highlighting potential false positives from standard diagnostics. Pathway analysis in proteogenomics-confirmed HER2+ samples identifies elevated epithelial-mesenchymal transition (EMT) and WNT-β-catenin signaling in non-pCR cases before treatment. Twenty-four pCR-associated proteins reproduce in a second proteomic dataset, and four (GPRC5A, TPBG, SP140L, and NEU1) are significant in a third. A meta-analysis of ten diverse neoadjuvant anti-HER2 treatment regimens from four independent studies confirms that non-pCR cases express higher levels of mRNA for G protein-coupled receptor class C group 5 member A (GPRC5A, p = 0.0002) and trophoblast glycoprotein (TPBG, p = 0.00008). Thus, proteogenomic analysis identifies negative biomarkers for pCR and alternative plasma membrane targets for treatment-resistant HER2+ breast cancer. This trial is registered at clinicaltrials.gov (NCT00770809).
Keywords: GPRC5A; HER2+; TPBG; anti-HER2 treatment; breast cancer; clinical trial; meta-analysis; neoadjuvant; proteogenomics; resistance.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests M.J.E. and C.M.P. are equity stockholders and consultants for Bioclassifier LLC. C.M.P. and M.J.E. are listed as inventors on issued and pending patents for the PAM50 subtyping assay. S.A.C. is a member of the scientific advisory boards of Kymera, PTM Biolabs, and Seer. M.A.G. and S.A.C. are members of the scientific advisory board of PrognomiQ. S.S. is currently employed by AstraZeneca, and AstraZeneca has no role in this study. M.A. and B.Z. received research funding from AstraZeneca, which played no role in this study, and B.Z. is a consultant for AstraZeneca and Inotiv. S.M.K. is a stakeholder in NeoZenome Therapeutics Inc. E.J.J., S.A.C., M.J.E., M.A.G., B.Z., and S.S. are co-inventors on a pending patent US20220326241A1 (Compositions and methods for treating cancer) from a previous HER2-focused study (Satpathy et al., 2020). M.J.E. was a full-time employee at AstraZeneca between March 2002 and March 2024 and is currently employed by Guardant Health, which had no role in this study.
Figures





References
-
- Cortazar P., Zhang L., Untch M., Mehta K., Costantino J.P., Wolmark N., Bonnefoi H., Cameron D., Gianni L., Valagussa P., et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384:164–172. doi: 10.1016/S0140-6736(13)62422-8. - DOI - PubMed
-
- Carey L.A., Berry D.A., Cirrincione C.T., Barry W.T., Pitcher B.N., Harris L.N., Ollila D.W., Krop I.E., Henry N.L., Weckstein D.J., et al. Molecular Heterogeneity and Response to Neoadjuvant Human Epidermal Growth Factor Receptor 2 Targeting in CALGB 40601, a Randomized Phase III Trial of Paclitaxel Plus Trastuzumab With or Without Lapatinib. J. Clin. Oncol. 2016;34:542–549. doi: 10.1200/JCO.2015.62.1268. - DOI - PMC - PubMed
-
- Fernandez-Martinez A., Krop I.E., Hillman D.W., Polley M.Y., Parker J.S., Huebner L., Hoadley K.A., Shepherd J., Tolaney S., Henry N.L., et al. Survival, Pathologic Response, and Genomics in CALGB 40601 (Alliance), a Neoadjuvant Phase III Trial of Paclitaxel-Trastuzumab With or Without Lapatinib in HER2-Positive Breast Cancer. J. Clin. Oncol. 2020;38:4184–4193. doi: 10.1200/JCO.20.01276. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U24 CA210954/CA/NCI NIH HHS/United States
- P50 CA058223/CA/NCI NIH HHS/United States
- U24 CA270823/CA/NCI NIH HHS/United States
- S10 OD028671/OD/NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U01 CA214125/CA/NCI NIH HHS/United States
- T32 GM136554/GM/NIGMS NIH HHS/United States
- R03 OD032626/OD/NIH HHS/United States
- U24 CA210986/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U24 CA196171/CA/NCI NIH HHS/United States
- U24 CA210979/CA/NCI NIH HHS/United States
- R01 CA229409/CA/NCI NIH HHS/United States
- P50 CA186784/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
