

Revealing differential psychotic symptoms in schizophrenia and bipolar I disorder by manifold learning and network analyses
- PMID: 40481013
- PMCID: PMC12144236
- DOI: 10.1038/s41398-025-03403-6
Revealing differential psychotic symptoms in schizophrenia and bipolar I disorder by manifold learning and network analyses
Abstract
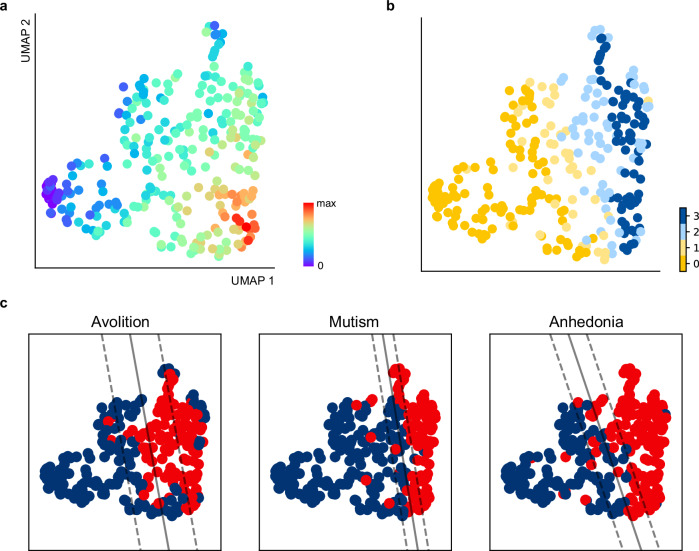
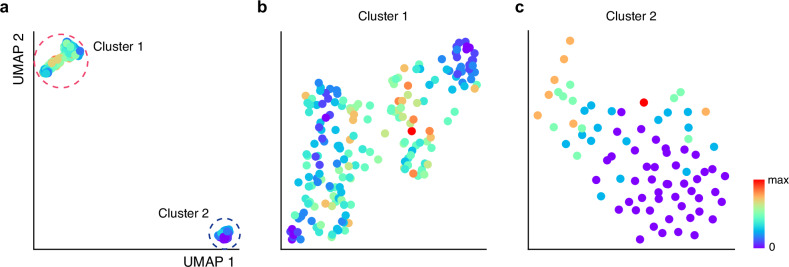
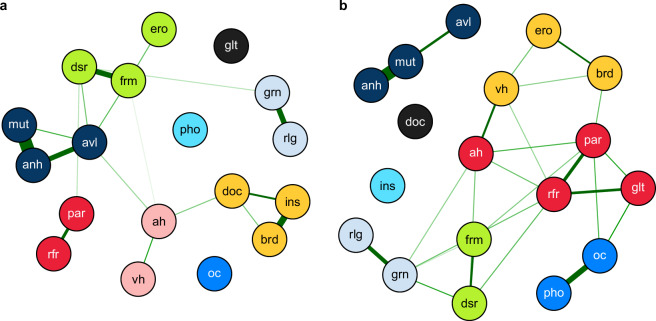
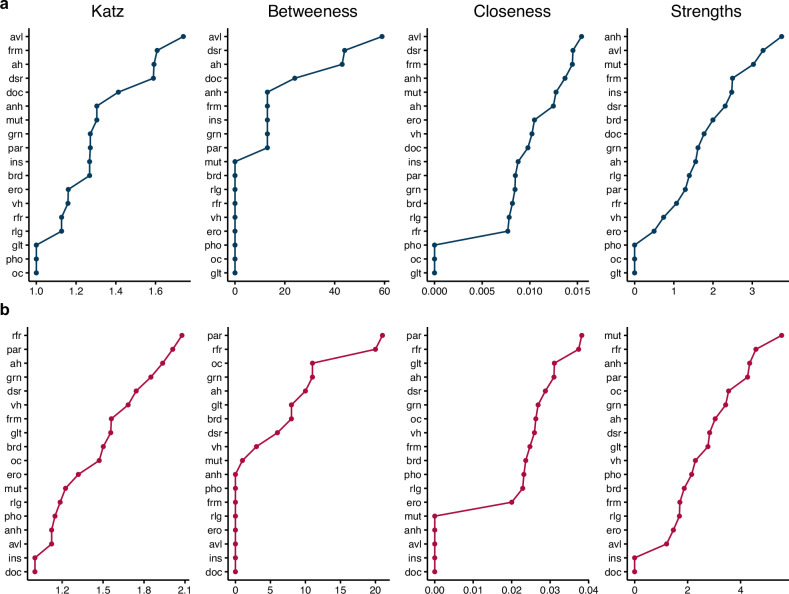
The field of psychiatry has encountered ongoing challenges in understanding the intricate nature of psychotic symptoms, particularly when they manifest in individuals diagnosed with bipolar disorder or schizophrenia. In this study, we employed manifold and network analyses to investigate whether the pattern of symptom occurrence differs between schizophrenia and bipolar I disorder. We analyzed data collected from 555 individuals, 282 of whom were diagnosed with schizophrenia-related disorders and 273 with bipolar I disorder. In the context of schizophrenia, negative symptoms, particularly avolition, were prominent with manifold and network analyses, identifying avolition as a high central symptom associated with clozapine use, patterns of deterioration, tendency toward remission, and illness severity. Conversely, bipolar I disorder exhibits discernible patterns where positive symptoms play a central role in network analysis. Unexpectedly, manifold analysis revealed two distinct clusters of patients, suggesting variability in psychotic symptom profiles within bipolar I disorder. In conclusion, schizophrenia and bipolar I disorder, while sharing psychotic symptoms, exhibit distinct co-occurrence patterns. Schizophrenia demonstrates negative symptoms, whereas bipolar I disorder exhibits a stronger interconnectivity of psychotic symptoms, highlighting the complexity of psychotic symptom patterns and their relevance for understanding psychiatric disorders. These findings highlight the complexity of psychotic symptom patterns and their relevance for understanding psychiatric disorders.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests. Ethical approval: The study was approved by the Institutional Review Board of Seoul National University Hospital (approval no.: 0106-080-002), and all participants provided written informed consent in accordance with the Declaration of Helsinki and relevant institutional guidelines. All methods were performed in accordance with the relevant guidelines and regulations.
Figures
References
-
- Pearlson GD. Etiologic, phenomenologic, and endophenotypic overlap of schizophrenia and bipolar disorder. Annu Rev Clin Psychol. 2015;11:251–81. - PubMed
-
- Lake CR. Schizophrenia and bipolar disorder: no dichotomy, a continuum, or one disease? Part 2. Psychiatric Annals. 2010;40:1.
-
- Kraepelin E. Einf? hrung in die psychiatrische Klinik. Рипол Классик; 1916.
-
- Lehmann HE, Ban TA. The history of the psychopharmacology of schizophrenia. Can J Psychiatry. 1997;42:152–62. - PubMed
-
- Möller H-J. Systematic of psychiatric disorders between categorical and dimensional approaches: Kraepelin’s dichotomy and beyond. Eur Arch Psychiatry Clin Neurosci. 2008;258:48–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
