

Primary closure with self-disengaging biliary stent following laparoscopic CBD exploration in normal-diameter ducts: a propensity score matching study
- PMID: 40481100
- PMCID: PMC12144154
- DOI: 10.1038/s41598-025-04949-7
Primary closure with self-disengaging biliary stent following laparoscopic CBD exploration in normal-diameter ducts: a propensity score matching study
Abstract
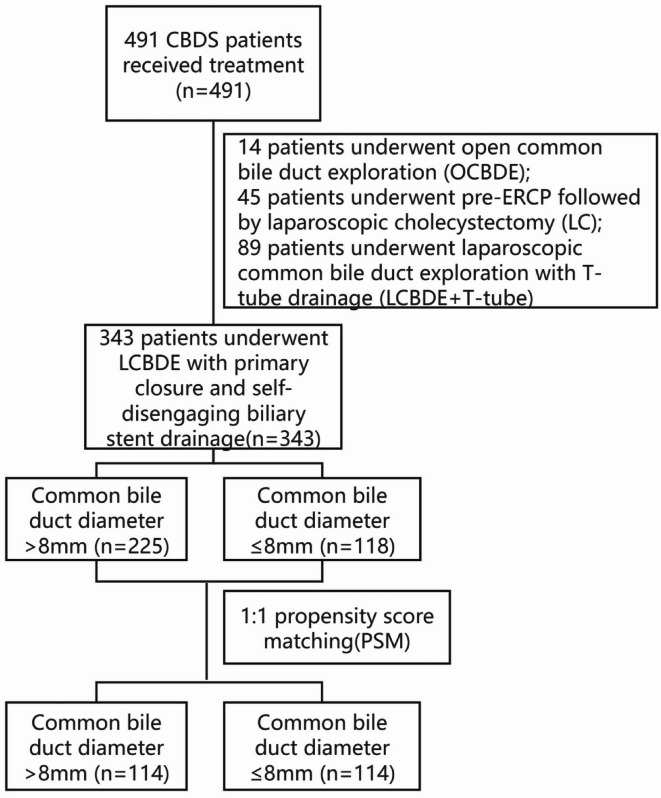
Laparoscopic Common Bile Duct Exploration (LCBDE) is highly effective for treating common bile duct stones (CBDS). This study aims to evaluate the safety and feasibility of primary closure with a self-disengaging biliary stent during LCBDE in patients with normal-diameter CBDs (≤ 8 mm) and to compare perioperative outcomes and complications with those in dilated CBDs (> 8 mm). From May 2022 to May 2024, patients with CBDSs who underwent LCBDE with primary closure and a self-disengaging biliary stent were retrospectively analyzed. Patients were stratified into two subgroups based on CBD diameter (normal: ≤8 mm vs. dilated: >8 mm). Propensity score matching (PSM) was adjusted for baseline differences between normal and dilated CBD groups, and perioperative indicators and postoperative complications were compared. Multivariate analysis identified risk factors for postoperative bile leakage. Of 491 patients, 343 underwent primary closure with a self-disengaging biliary stent during LCBDE. The mean operation time was 85 (IQR 70-110) min, with blood loss of 20 (IQR 15-20) ml. The postoperative hospital stay was 8 (IQR 8-10) days, and the hospitalization cost was CNY 28,143 (IQR 25,522-32,809). The overall complication rate was 32 (9.3%), with 25 (7.3%) experiencing bile leakage. The Charlson Comorbidity Index (CCI) score was an independent risk factor for bile leakage (OR 2.587; 95% CI 1.729-3.873, P < 0.001). PSM of dilated (> 8 mm, n = 225) and normal (≤ 8 mm, n = 118) CBD groups resulted in 114 matched pairs. No significant differences were observed in operative time, blood loss, hospital stay, costs, or complications between the groups. Primary closure with a self-disengaging biliary stent following LCBDE is equally safe and effective in patients with normal-diameter CBDs as in those with dilated ducts. CBD diameter should not be a contraindication for this technique. The CCI score is a critical predictor of bile leakage and should be considered in perioperative risk assessment.
Keywords: Bile leakage; Common bile duct stones (CBDSs); Laparoscopic common bile duct exploration (LCBDE); Primary closure; Self-disengaging biliary stent.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Efficacy and safety of laparoscopic common bile duct exploration via choledochotomy with primary closure for the management of acute cholangitis caused by common bile duct stones.Surg Endosc. 2022 Jul;36(7):4869-4877. doi: 10.1007/s00464-021-08838-8. Epub 2021 Nov 1. Surg Endosc. 2022. PMID: 34724579 Free PMC article.
-
Comparison of primary duct closure versus T-tube drainage in laparoscopic common bile duct exploration: a propensity score matching analysis.Surg Endosc. 2025 Apr;39(4):2481-2488. doi: 10.1007/s00464-025-11610-x. Epub 2025 Feb 24. Surg Endosc. 2025. PMID: 39994046
-
Laparoscopic common bile duct exploration in patients with previous abdominal biliary tract operations.Surg Endosc. 2020 Apr;34(4):1551-1560. doi: 10.1007/s00464-020-07429-3. Epub 2020 Feb 18. Surg Endosc. 2020. PMID: 32072280 Free PMC article.
-
Laparoscopic common bile duct exploration.Surg Endosc. 2003 Nov;17(11):1705-15. doi: 10.1007/s00464-002-8917-4. Epub 2003 Sep 10. Surg Endosc. 2003. PMID: 12958681 Review.
-
Laparoscopic common bile duct exploration plus cholecystectomy versus endoscopic retrograde cholangiopancreatography plus laparoscopic cholecystectomy for cholecystocholedocholithiasis: a meta-analysis.Surg Endosc. 2019 Oct;33(10):3275-3286. doi: 10.1007/s00464-018-06613-w. Epub 2018 Dec 3. Surg Endosc. 2019. PMID: 30511313 Review.
References
-
- Tanase, A., Dhanda, A., Cramp, M., Streeter, A. & Aroori, S. A UK survey on variation in the practice of management of choledocholithiasis and laparoscopic common bile duct exploration (ALiCE Survey). Surg. Endosc. 36, 5882–5896 (2022). - PubMed
-
- Chen, A. P. et al. Clinical dfficacy of primary closure in laparoscopic common bile duct exploration (a report of 2429 cases). Chin. J. Dig. Surg.17, 299–303 (2018).
-
- Dasari, B. V. et al. Surgical versus endoscopic treatment of bile duct stones. Cochrane Database Syst. RevCD003327 (2013). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
