

Fluorescence-guided ureteral identification in robotic surgery for advanced endometriosis: a comparison of junior versus senior surgeons
- PMID: 40481106
- PMCID: PMC12144151
- DOI: 10.1038/s41598-025-05082-1
Fluorescence-guided ureteral identification in robotic surgery for advanced endometriosis: a comparison of junior versus senior surgeons
Abstract
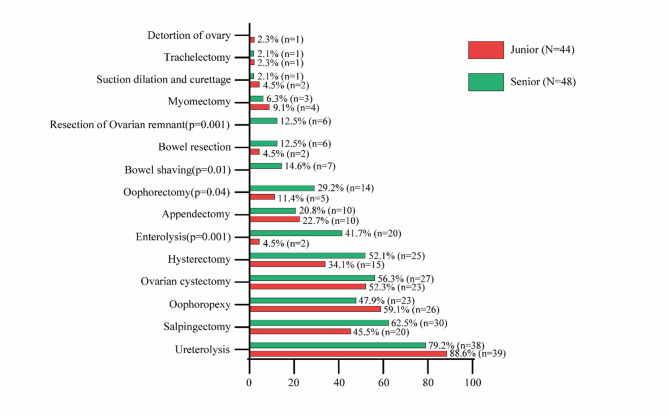
Identifying the ureters in patients with advanced endometriosis and severe pelvic adhesive disease can be challenging. Adhesiolysis along the deformed pelvic sidewall may increase the risk of prolonged operative time and incidental ureteral injury. This study aimed to evaluate the safety and surgical outcomes of using Indocyanine Green (ICG) under near-infrared fluorescence for intraoperative ureteral localization and preservation during robot-assisted laparoscopic surgery (RALS) for advanced endometriosis, comparing procedures performed by two junior surgeons to those performed by one senior surgeon. This was a retrospective observational case series conducted by three minimally invasive gynecologic surgeons (X.G., T.K., B.T.) at a single tertiary care center between August 2021 and January 2025. A total of 92 patients underwent RALS using ICG fluorescence; 44 surgeries were performed by two junior surgeons, and 48 by a senior surgeon. The senior group had a higher percentage of patients with complete cul-de-sac obliteration (56.3% vs. 18.2%, p = 0.001). Our primary surgical outcome, total operative time, was 233 min in the junior group and 348 min in the senior group, initially showing a significant difference. However, after adjusting for factors such as history of prior abdominal surgery, cul-de-sac obliteration, and additional procedures (resection of ovarian remnant, bowel shaving, oophorectomy, enterolysis) using multivariable linear regression analysis, no significant difference was observed between the two groups. Other perioperative outcomes-including patient characteristics, estimated blood loss, length of hospital stay, and postoperative pain at weeks 1, 2, and 3-were comparable between the groups. Complication rates did not differ significantly. Notably, there were no cases of temporary or permanent ureteral injury in either group. These findings suggest that with ICG-assisted ureteral mapping, junior surgeons can achieve comparable surgical outcomes to senior surgeons. ICG facilitates intraoperative ureter identification, with the potential to enhance surgical safety by improving surgical precision and supporting the training of junior surgeons in managing complex endometriosis.
Keywords: Advanced-stage endometriosis; Fluorescence; Robot-assisted laparoscopic surgery; Ureteral identification.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: The need for consent to participate was waived due to retrospective nature of the study by an Institutional Review Board (IRB). This study was IRB-approved from Baylor College of Medicine on March 8, 2022, under the approval number H-51429.
Figures
Similar articles
-
Indocyanine green near-infrared fluorescence bowel perfusion assessment to prevent anastomotic leakage in minimally invasive colorectal surgery (AVOID): a multicentre, randomised, controlled, phase 3 trial.Lancet Gastroenterol Hepatol. 2024 Oct;9(10):924-934. doi: 10.1016/S2468-1253(24)00198-5. Epub 2024 Aug 13. Lancet Gastroenterol Hepatol. 2024. PMID: 39151436 Clinical Trial.
-
Surgical interventions for the management of chronic pelvic pain in women.Cochrane Database Syst Rev. 2021 Dec 20;12(12):CD008212. doi: 10.1002/14651858.CD008212.pub2. Cochrane Database Syst Rev. 2021. PMID: 34923620 Free PMC article.
-
Laparoscopy and robotic-assisted surgery for endometriosis: how intestinal and ovarian involvement impact operative time.J Robot Surg. 2025 Jul 24;19(1):417. doi: 10.1007/s11701-025-02588-8. J Robot Surg. 2025. PMID: 40705127
-
Laparoscopic surgery for elective abdominal aortic aneurysm repair.Cochrane Database Syst Rev. 2017 May 4;5(5):CD012302. doi: 10.1002/14651858.CD012302.pub2. Cochrane Database Syst Rev. 2017. PMID: 28471523 Free PMC article.
-
The Use of near Infra-Red Radiation Imaging after Injection of Indocyanine Green (NIR-ICG) during Laparoscopic Treatment of Benign Gynecologic Conditions: Towards Minimalized Surgery. A Systematic Review of Literature.Medicina (Kaunas). 2022 Jun 13;58(6):792. doi: 10.3390/medicina58060792. Medicina (Kaunas). 2022. PMID: 35744056 Free PMC article.
References
-
- Zhu, Y. et al. Identification of potential diagnostic biomarkers and drug targets for endometriosis from a genetic perspective: a Mendelian randomization study. Gynecol. Obstet. Investig.10.1159/000543707 (2025). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
