

Immune age is correlated with decreased TCR clonal diversity and antibody response to SARS-CoV-2
- PMID: 40481111
- PMCID: PMC12144168
- DOI: 10.1038/s41598-025-04736-4
Immune age is correlated with decreased TCR clonal diversity and antibody response to SARS-CoV-2
Abstract
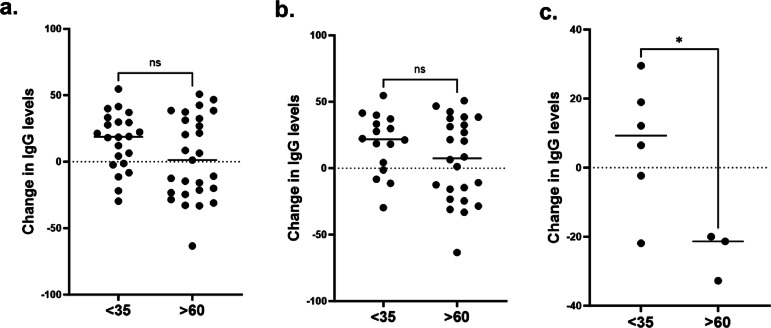
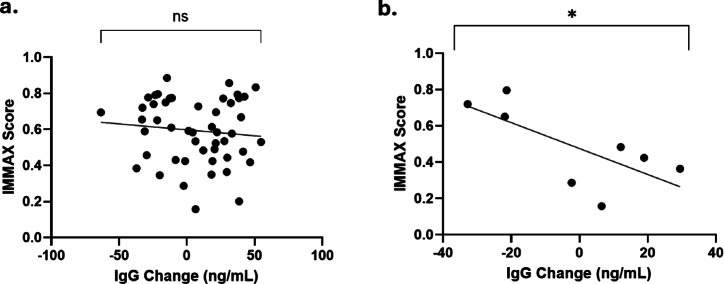
Immune response to infection or vaccination is compromised with age. We aimed to examine associations between immune senescence, T and B cell clonal diversity and immunoglobulin G secretion in response to immune challenge in isolated peripheral blood mononuclear cells (PBMC) from people of different chronological ages. We isolated PBMC from 49 individuals categorised into < 35 years and > 60 years age groups. Cells were then challenged with recombinant SARS-CoV-2 spike protein or vehicle and IMMAX score was calculated for each sample from flow cytometry. Antibody response was assessed using the proxy of IgG secretion and T cell receptor and immunoglobulin framework region recombination was determined by clonality studies. We observed that individuals aged > 60 years demonstrated a higher immune 'age' as calculated by IMMAX score (0.75 compared with 0.48 for individuals aged < 35 years; p = < 0.0001). Immune age negatively correlated with IgG responsivity in older individuals with recent prior exposure to SARS-CoV-2 (b = -0.01; p = 0.05). Higher immune age was also negatively correlated with TCR Vd + Jd receptor diversity regardless of immune challenge (b = -0.02; p = < 0.0001 and b = -0.02; r2 = 0.0.35; p = < 0.0001 for control and exposed samples respectively). Our data demonstrate that PBMC samples from older people display a higher cellular immune age and attenuation of immune response. This suggests that future treatments targeting cellular ageing of immune cells may be a useful avenue for investigation to improve immune function in older people.
Keywords: Immune age; Immune function; SARS-CoV-2; Senescence; T cell.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: LWH is Founder, Director and Chief Scientific Officer for SENISCA Ltd. Merlin Davies now works for SENISCA, but did not do so at the time this work was undertaken. HD is project lead for data science at SENISCA Ltd. The work described in this publication has no relationship with or bearing on SENISCA’s activities. All the remaining authors declare no conflict of interest.
Figures




References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
