

Two cases of Talaromyces marneffei tracheobronchial infection in HIV-negative patients
- PMID: 40481394
- PMCID: PMC12144829
- DOI: 10.1186/s12879-025-11143-7
Two cases of Talaromyces marneffei tracheobronchial infection in HIV-negative patients
Erratum in
-
Correction: Two cases of Talaromyces Marneffei tracheobronchial infection in HIV-negative patients.BMC Infect Dis. 2025 Jun 26;25(1):809. doi: 10.1186/s12879-025-11239-0. BMC Infect Dis. 2025. PMID: 40571937 Free PMC article. No abstract available.
Abstract
Objectives: In recent years, the incidence and prevalence of Talaromyces marneffei (TM) have been on the rise. This infection predominantly affects immunocompromised or immunodeficient individuals, especially those with acquired immunodeficiency syndrome (AIDS). There has been a notable increase in the incidence of TM and its associated infections. The majority of cases occur within immunocompromised or immunodeficient populations, with a high prevalence among AIDS patients. However, cases are also occasionally detected in HIV - negative individuals. Due to the insidious and slow - growing nature of TM, the disease can be misdiagnosed as other conditions such as tuberculosis, bacterial pneumonia, and lung cancer, particularly in non - endemic regions. Such misdiagnosis significantly impacts the patient’s prognosis.
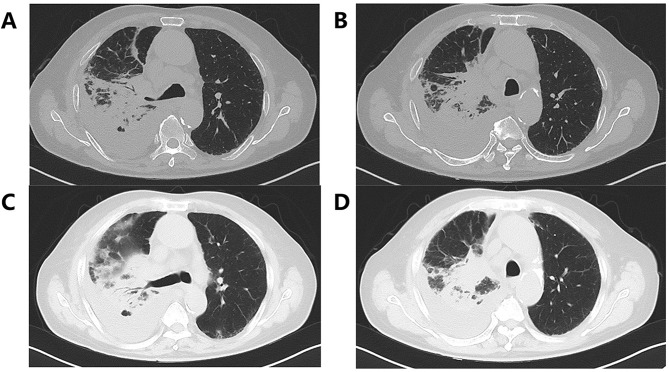
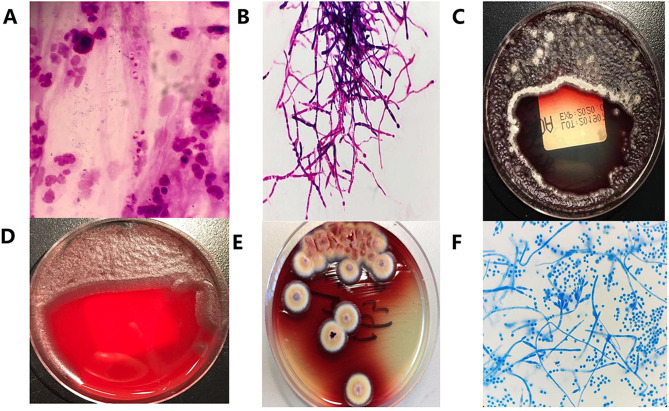
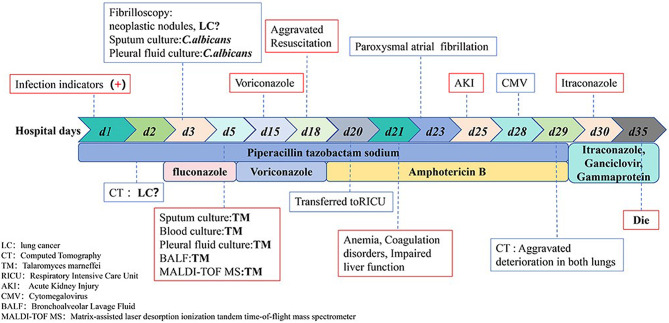
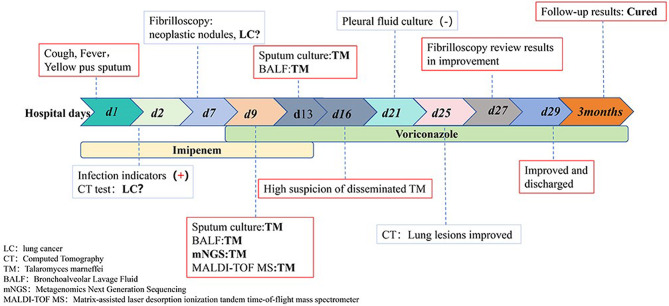
Methods: Two HIV-negative patients with TM infection from non - endemic areas were hospitalized with a high suspicion of co-infection with lung cancer and poor symptomatic treatment response. These patients underwent a comprehensive diagnostic workup, including lung puncture biopsy, sputum, blood, pleural, and peritoneal fluid cultures, as well as Metagenomics Next Generation Sequencing (mNGS) analysis. Eventually, both patients were diagnosed with TM tracheobronchial infection.
Results: The patients were treated with voriconazole antifungal therapy, combined with methylprednisolone (used for reducing inflammation, relieving spasms, and treating asthma) and acyclovir (used for treating viral infections). The 49 - year - old patient was cured and discharged from the hospital, while the 79 - year - old male patient’s condition continued to deteriorate, and he ultimately died.
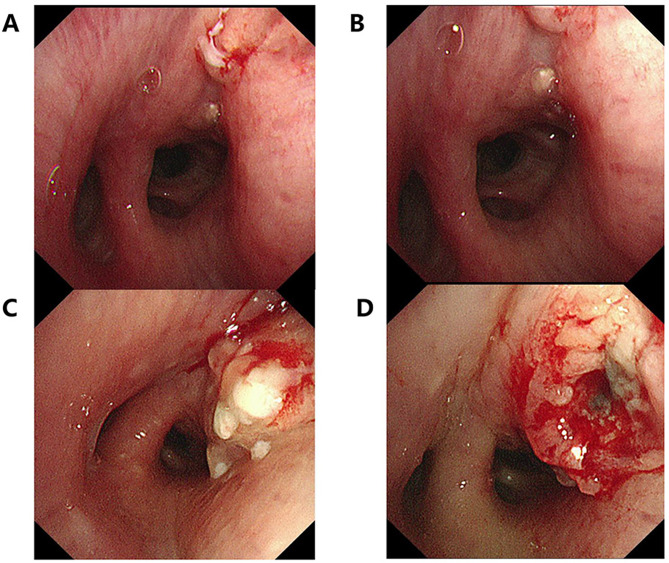
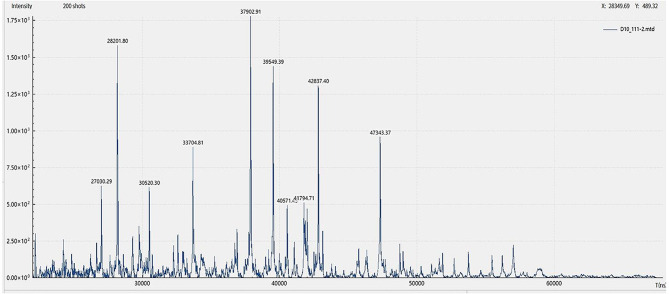
Conclusion: It has been determined that TM infection, presenting primarily with respiratory symptoms, is highly susceptible to misdiagnosis in the early stages of the disease. This can lead to treatment delays and a negative impact on the prognosis. It is crucial for medical professionals to be more aware of the possibility of TM infection in non - HIV - infected and non - endemic populations. Collecting respiratory and lung tissue specimens from the infection sites at the earliest possible stage is essential for diagnosing TM infection. Integrating mNGS and mass spectrometry results is crucial for improving the detection and early diagnosis of TM infection, which is of great value for enhancing the efficacy of clinical treatment and the prognosis of patients.
Clinical trial number: Not applicable.
Keywords: Talaromyces marneffei; Antifungal therapy; HIV-negative patient; Tracheobronchial infection.
Conflict of interest statement
Declarations. Ethics approval and informed consent: The documentation and publication of the case were approved by the Ethics Review Committee of West China Hospital, Sichuan University (Approval Number: 20231974). Written informed consent for the publication of their details was obtained from the patients. The subjects’ rights were adequately protected, and there was no potential risk to the subjects. Consent for publication: The present study has confirmed that the participant/patient has provided written informed consent for the publication of their personal or clinical details and any identifiable images in this study. For case 1 patient who has passed away, written informed consent has also been obtained from his family.All authors thank the patient and his family members for allowing us to understand her condition and write this case report.All authors agreed on the journal in which the article was to be submitted and unanimously agreed to publish it. Competing interests: The authors declare no competing interests.
Figures
References
-
- Deng ZL, Yun M, Ajello L. Human penicilliosis Marneffei and its relation to the bamboo rat (Rhizomys pruinosus)[J]. J Med Vet Mycol. 1986;24(5):383–9. 10.1080/02681218680000581. - PubMed
-
- Limper AH, Adenis A, Le T, et al. Fungal infections in HIV/AIDS[J]. Lancet Infect Dis. 2017;17(11):e334–43. 10.1016/S1473-3099(17)30303-1. - PubMed
LinkOut - more resources
Full Text Sources
