

The clinical practice and outcomes of minimally invasive surgery in primary malignant melanoma of the vagina and cervix patients: a retrospective cohort study
- PMID: 40481497
- PMCID: PMC12144728
- DOI: 10.1186/s13023-025-03760-x
The clinical practice and outcomes of minimally invasive surgery in primary malignant melanoma of the vagina and cervix patients: a retrospective cohort study
Abstract
Background: Primary malignant melanoma of the vagina (PMMV) and cervix (PMMC) are extremely rare tumors with a poor prognosis, lacking well-defined protocols or standardized treatment guidelines. While the preferred management for early-stage PMMV and PMMC is surgery, comprehensive reports on the impact of various surgical techniques on cancer outcomes are scarce.
Objective: This study aimed to compare outcomes between open and minimally invasive surgery (MIS) in PMMV and PMMC, and concurrently evaluated prognostic risk factors for these conditions.
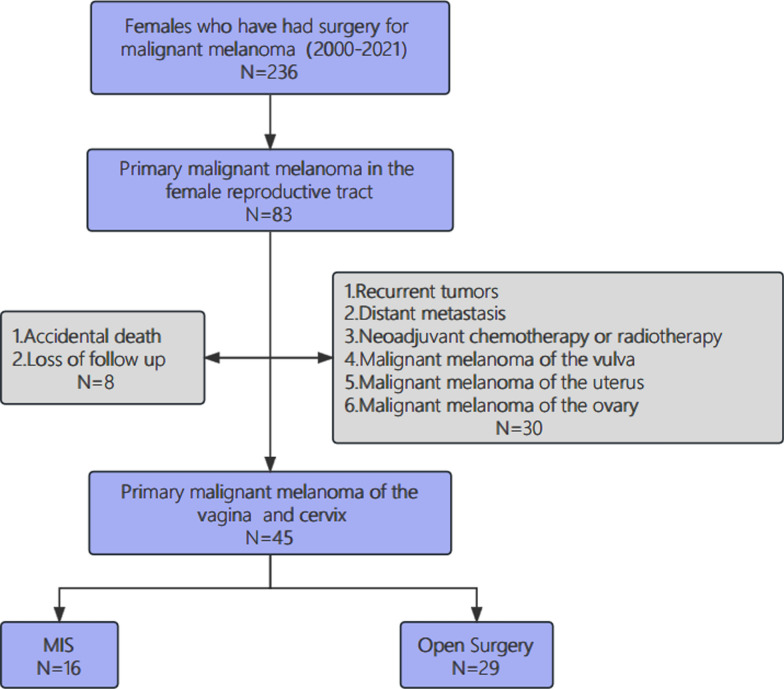
Methods: We conducted a single-center retrospective cohort study of PMMV and PMMC patients treated surgically from January 2000 to July 2021. Clinicopathological features and surgical outcomes were assessed retrospectively. Patients underwent either open surgery or MIS. Disease-Free Survival (DFS) rates were compared.
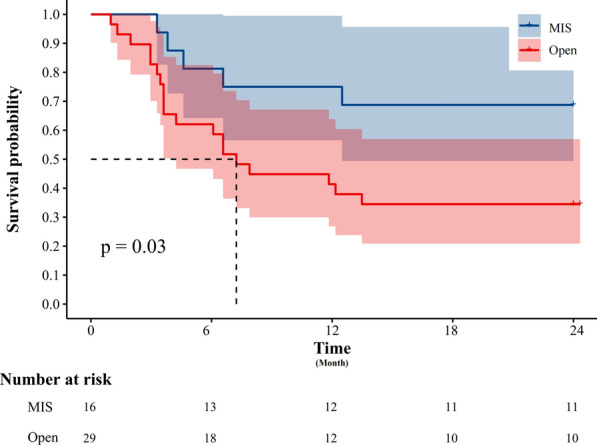
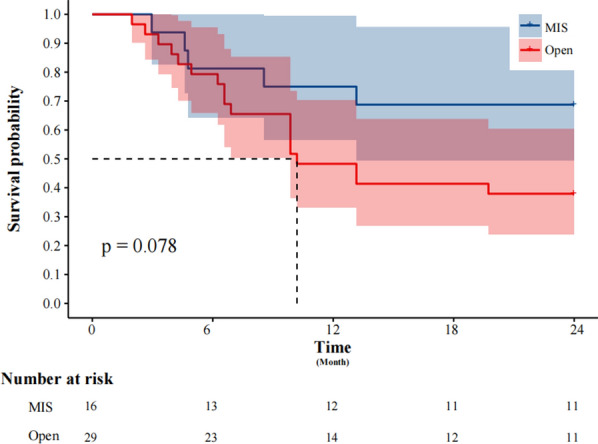
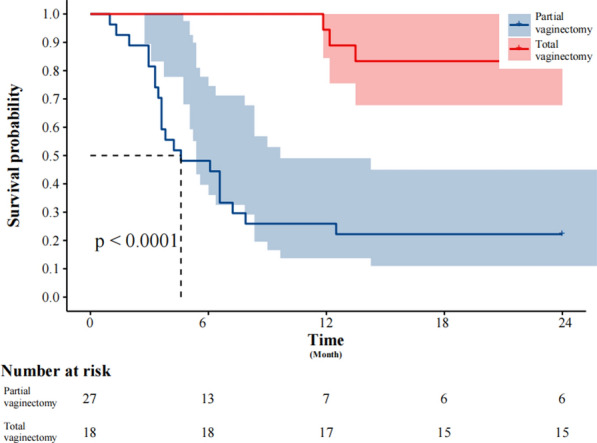
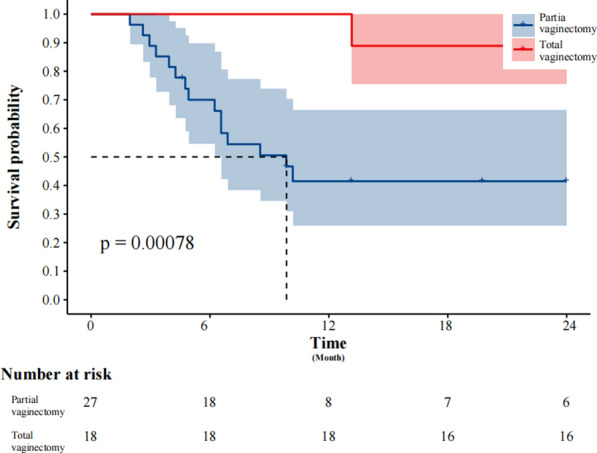
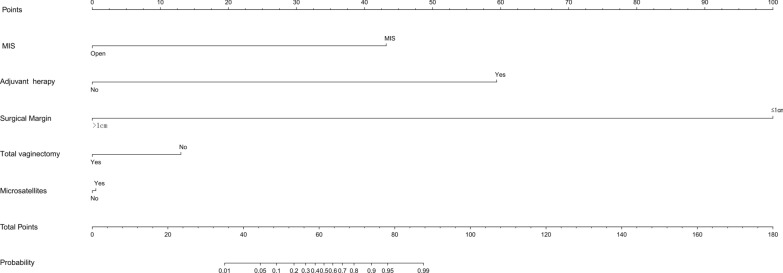
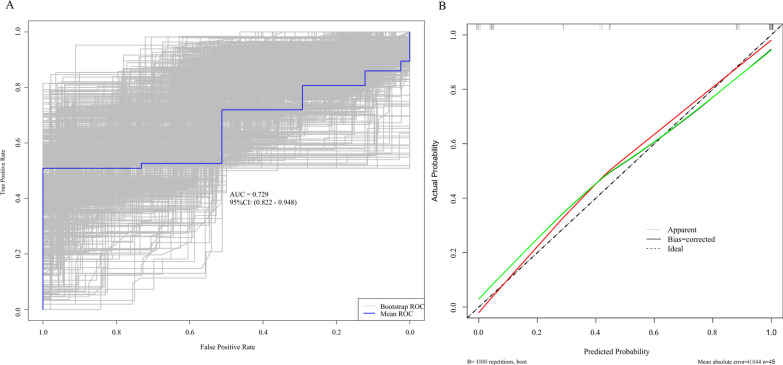
Results: Of 45 eligible patients, the MIS group showed a higher rate of total vaginectomy (P = 0.022), reduced median intraoperative blood loss (P = 0.031), shorter median hospital stay (P = 0.042), and no significant increase in perioperative complications (P = 0.867). The incidence of negative margins < 1 cm was significantly lower in the MIS group (P = 0.032). Cox proportional hazards regression identified microsatellites (HR = 2.893 [1.042-8.029]; P = 0.042), surgical negative margin distance (HR = 0.042 [0.008-0.217]; P < 0.001), and total vaginectomy (HR = 0.042 [0.008-0.217]; P < 0.001) as independent prognostic factors for DFS. MIS was linked to a significant difference in 2-year DFS (P = 0.030), but there was no notable difference in overall survival (OS) compared to open surgery (P = 0.078). The outcomes are validated through sensitivity analysis and hierarchical assessment, leading to the development of a novel nomogram simultaneously.
Conclusions: Total vaginectomy may improve DFS in PMMV and PMMC patients. A combination of MIS and radical vaginal resection can effectively manage PMMV and PMMC as an initial surgical strategy.
Keywords: Minimally invasive surgery; Outcomes; Primary malignant melanoma of the cervix; Primary malignant melanoma of the vagina; Rare diseases.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Fujian Cancer Hospital’s ethics committee on September 10, 2023. Approval number: K2023-246–01. Consent for publication: Not applicable. Competing interests: The authors have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Sinasac SE, Petrella TM, Rouzbahman M, Sade S, Ghazarian D, Vicus D. Melanoma of the Vulva and Vagina: surgical management and outcomes based on a clinicopathologic review of 68 cases. J Obstet Gynaecol Can. 2019;41(6):762–71. - PubMed
-
- Irvin WP Jr, Legallo RL, Stoler MH, Rice LW, Taylor PT Jr, Andersen WA. Vulvar melanoma: a retrospective analysis and literature review. Gynecol Oncol. 2001;83(3):457–65. - PubMed
-
- Verschraegen CF, Benjapibal M, Supakarapongkul W, Levy LB, Ross M, Atkinson EN, et al. Vulvar melanoma at the M. D. Anderson Cancer Center: 25 years later. Int J Gynecol Cancer. 2001;11(5):359–64. - PubMed
-
- Weinstock MA. Malignant melanoma of the vulva and vagina in the United States: patterns of incidence and population-based estimates of survival. Am J Obstet Gynecol. 1994;171(5):1225–30. - PubMed
