

Lateral position posterior surgery followed by supine position anterior surgery in a single stage (LP-A) for the treatment of cervical spinal cord anterior severe dynamic compression in short-term
- PMID: 40481551
- PMCID: PMC12143083
- DOI: 10.1186/s13018-025-05976-w
Lateral position posterior surgery followed by supine position anterior surgery in a single stage (LP-A) for the treatment of cervical spinal cord anterior severe dynamic compression in short-term
Abstract
Purpose: To evaluate the effectiveness and safety of the lateral position posterior surgery ahead of the anterior surgery (LP-A) in a single stage for releasing the cervical spinal cord from short-term severe anterior compression.
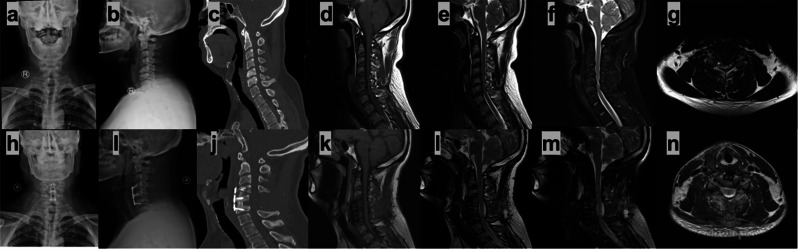
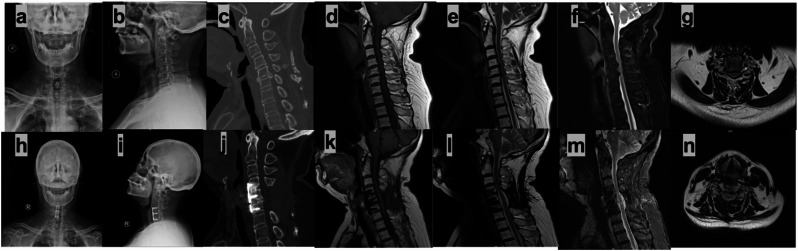
Methods: The severe stenosis with dynamic compression defined as Vaccaro`s system degree 3 or 4 with neurological symptoms aggravation when flexion or extension of the cervical spine. Retrospectively analyzed 64 short-level degenerative cervical myelopathy (DCM) patients from severe compression who underwent posterior cervical decompression in the lateral position ahead of supine anterior decompression and fusion at a single stage.
Results: Sixty-four patients with DCM from severe compression were enrolled. The mean operation time was 183.06 ± 32.42 min. The postoperative mJOA scores of the patients increased from 7.61 ± 0.94 to 14.03 ± 0.78. The expansion degree of the cervical spinal cross-sectional area and drift-back distance rose from 62.05 ± 14.05 to 164.05 ± 37.62mm2 and from 5.08 ± 1.22 to 12.70 ± 1.26, respectively. The Neck Disability Index was 31.81 ± 3.17 before the operation, 20.14 ± 2.22, 17.69 ± 1.56, 15.64 ± 1.51, and 13.70 ± 1.50 at 1, 3, 6, and 12 months after the operation, respectively. The visual analogue scale (VAS) score of the cervical was 5.64 ± 1.01 before the operation, 2.41 ± 0.64, 2.08 ± 0.48, 1.45 ± 0.50, and 1.06 ± 0.47 at 1, 3, 6, and 12 months after the operation, respectively. The sagittal vertical axis (cSVA) and the Cobb angle were significantly changed after surgery.
Conclusion: Posterior cervical decompression in the lateral position ahead of anterior decompression and fusion in a single stage is an effective and safe surgical procedure for the treatment of severe short-term cervical cord anterior compression.
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
[Combined cervical posterior-anterior operation for treatment of cervical spinal canal stenosis with reverse arch].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013 Apr;27(4):385-8. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013. PMID: 23757860 Chinese.
-
Extrinsic thoracic spinal cord compression related to supine position: from diagnosis to the creation of a spinal protection shield.Spine J. 2016 Jan 1;16(1):117-22. doi: 10.1016/j.spinee.2015.09.041. Epub 2015 Sep 28. Spine J. 2016. PMID: 26416266
-
Anterior Cervical Controllable Antedisplacement and Fusion (ACAF): Improving Outcomes for Severe Cervical Ossification of the Posterior Longitudinal Ligament.JBJS Essent Surg Tech. 2022 May 19;12(2):e20.00056. doi: 10.2106/JBJS.ST.20.00056. eCollection 2022 Apr-Jun. JBJS Essent Surg Tech. 2022. PMID: 36741044 Free PMC article.
-
Spinal exposure for anterior lumbar interbody fusion (ALIF) in the lateral decubitus position: anatomical and technical considerations.Eur Spine J. 2022 Sep;31(9):2188-2195. doi: 10.1007/s00586-022-07227-6. Epub 2022 May 12. Eur Spine J. 2022. PMID: 35552530 Review.
References
-
- Nouri A, Tetreault L, Singh A, Karadimas SK, Fehlings MG. Degenerative cervical myelopathy: epidemiology, genetics, and pathogenesis. Spine (Phila Pa 1976). 2015;40(12):E675–93. - PubMed
-
- Robertson SC, Ashley MR. Complications of anterior cervical discectomy and fusion. Acta Neurochir Suppl. 2023;130:169–78. - PubMed
-
- Fountas KN, Kapsalaki EZ, Nikolakakos LG, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976). 2007;32(21):2310–7. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
