

How does the dual policy-the C-DRG-based reimbursement system and subsidy policy for appropriate Traditional Chinese Medicine (TCM) techniques-influence physicians' choice of disease treatment methods in TCM hospitals?
- PMID: 40481925
- PMCID: PMC12144693
- DOI: 10.1186/s13561-025-00643-6
How does the dual policy-the C-DRG-based reimbursement system and subsidy policy for appropriate Traditional Chinese Medicine (TCM) techniques-influence physicians' choice of disease treatment methods in TCM hospitals?
Abstract
Background: This study investigates the impact of the diagnosis-related group (DRG) reimbursement system and subsidy policies on the treatment methods of traditional Chinese medicine (TCM) orthopaedic physicians. The objective is to determine the optimal subsidy amount to maximize the number of treated patients.
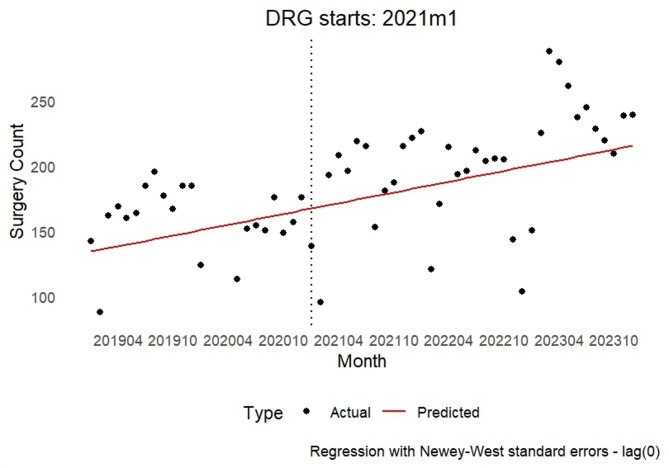
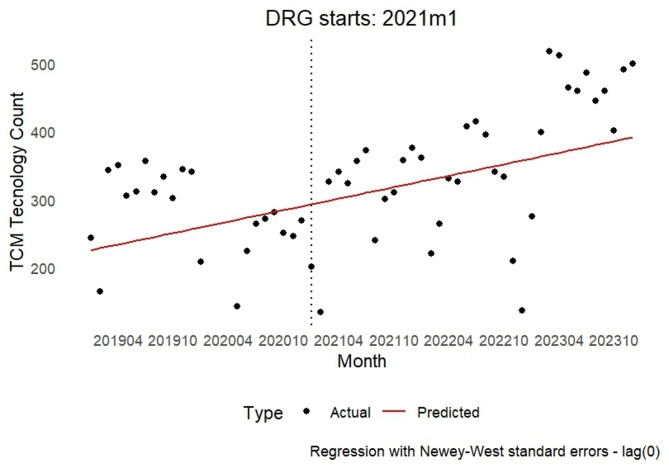
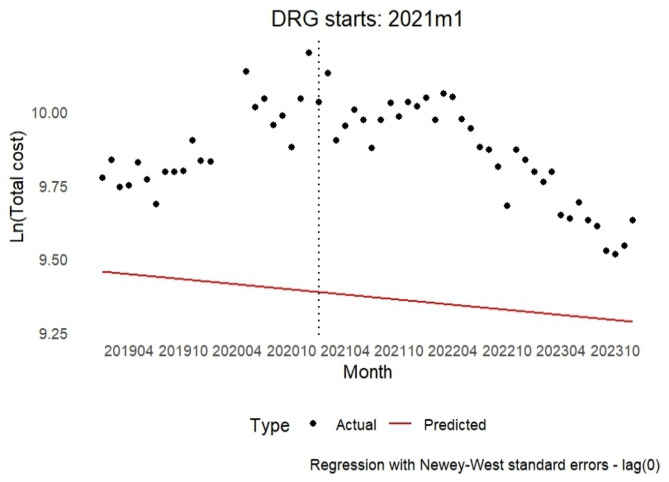
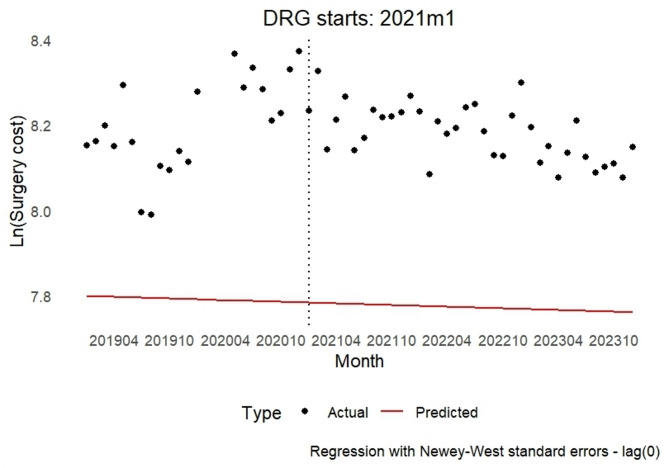
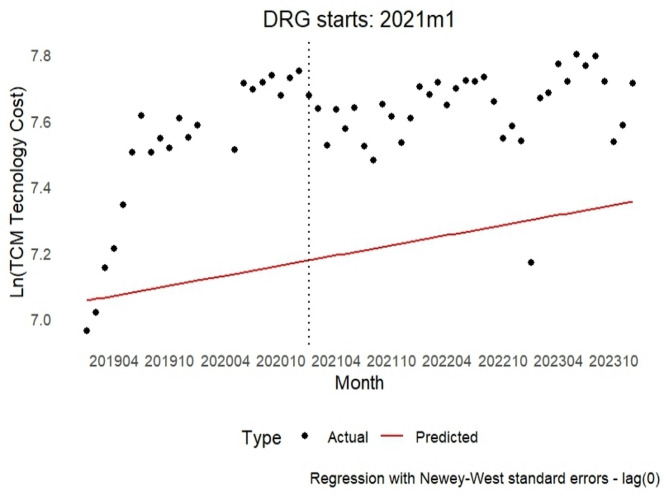
Methods: Using Evans' profit maximization theory, the study examines the intrinsic motivations behind physicians' behaviours and their influence on the medical market. A discontinuous time series analysis evaluates the effects of the C-DRG-based reimbursement system and subsidies on the number of treated inpatients and inpatient expenses in TCM orthopaedics.
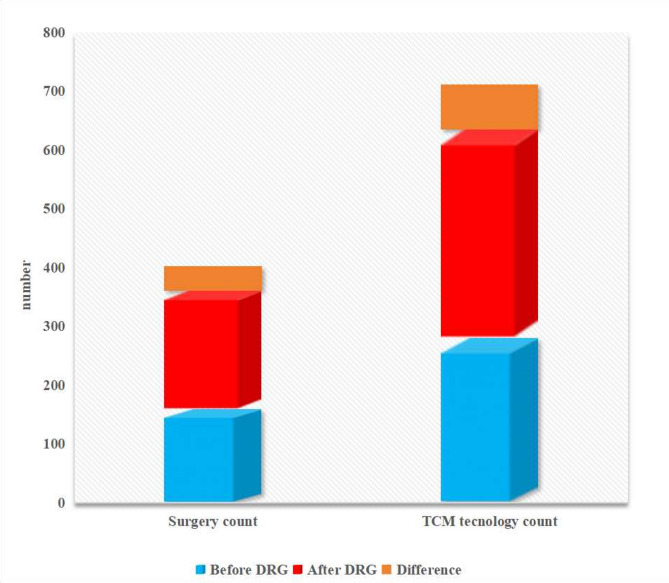
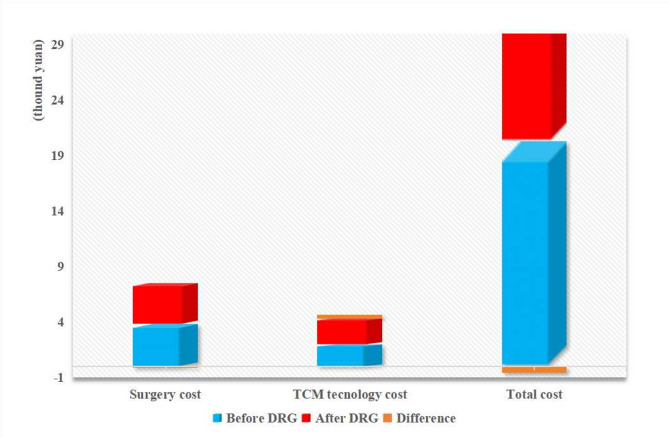
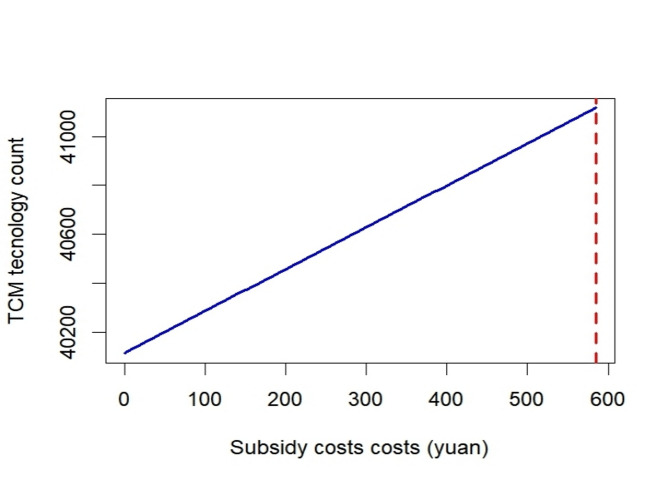
Results: The expanded implementation of the C-DRG-based reimbursement system substantially boosted both orthopaedic surgery and TCM technology case volumes, with 55 additional orthopaedic procedures and 200 extra TCM interventions recorded (p < 0.001).Total and surgical expenses decreased notably by 42.7% and 26.29%, respectively(p < 0.001), while inpatient expenses for TCM techniques decreased significantly by 32.63% (p < 0.05). Subsidy policies during the C-DRG-based reimbursement system implementation significantly increased the use of appropriate TCM techniques without substantially impacting total expenses. Physicians partially achieved both DRG expenses control and subsidy policy objectives by reducing total expenses and increasing TCM technique usage. The optimal subsidy amount was calculated to be 584.79 RMB, showing a linear relationship with TCM orthopaedic cases, with peak usage aligning with optimal subsidy timing.
Conclusion: The C-DRG-based reimbursement system and subsidy policies positively influenced the treatment methods of TCM orthopaedic physicians, increasing the number of treated cases and reducing expenses. An optimal subsidy of 584.79 RMB was identified to maximize the number of treated patients, aligning with both DRG expenses control and subsidy policy objectives.
Keywords: Appropriate Traditional Chinese Medicine (TCM) techniques; Diagnosis-Related Group (DRG) payment system; Interrupted time series analysis (ITS); Optimal subsidy expenses value; Policy impact.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: Not applicable. Consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Do the diagnosis-related group payment reforms have a negative impact?-an empirical study from Western China.Front Public Health. 2025 Apr 11;13:1550480. doi: 10.3389/fpubh.2025.1550480. eCollection 2025. Front Public Health. 2025. PMID: 40290505 Free PMC article.
-
The impact of DRG on resource consumption of inpatient with ischemic stroke.Front Public Health. 2023 Nov 7;11:1213931. doi: 10.3389/fpubh.2023.1213931. eCollection 2023. Front Public Health. 2023. PMID: 38026323 Free PMC article.
-
A study of the types and manifestations of physicians' unintended behaviors in the DRG payment system.Front Public Health. 2023 Jun 27;11:1141981. doi: 10.3389/fpubh.2023.1141981. eCollection 2023. Front Public Health. 2023. PMID: 37441652 Free PMC article.
-
The impact of diagnosis-related group-based medical insurance payment model on the prognosis and nursing care of patients undergoing composite trabeculectomy: a retrospective cohort study.Front Public Health. 2025 May 21;13:1518546. doi: 10.3389/fpubh.2025.1518546. eCollection 2025. Front Public Health. 2025. PMID: 40469599 Free PMC article. Review.
-
Is There An Association Between Bundled Payments and "Cherry Picking" and "Lemon Dropping" in Orthopaedic Surgery? A Systematic Review.Clin Orthop Relat Res. 2021 Nov 1;479(11):2430-2443. doi: 10.1097/CORR.0000000000001792. Clin Orthop Relat Res. 2021. PMID: 33942797 Free PMC article.
References
-
- Chalkley M, Malcomson J. Contracting for health services when patient demand does not reflect quality. J Health Econ. 1998;17(1):1–19. 10.1016/S0167-6296(97)00019-2. - PubMed
-
- Chalkley M, Malcomson J. Expenses sharing in health service provision: an empirical assessment of expenses savings. J Public Econ. 2002;84(2):219–49. 10.1016/S0047-2727(01)00126-8.
-
- Ehrlich I, Becker GS. Market insurance, Self-Insurance, and Self-Protection. J Polit Econ. 1972;80(4):623–48. https://www.journals.uchicago.edu/doi/abs/10.1086/259916. - DOI
-
- Fuchs VR. The supply of surgeons and the demand for operations. J Hum Resour. 1978;13(236):35–56. https://www.nber.org/papers/w0236. - PubMed
-
- Ellis R, McGuire T. Provider behavior under prospective reimbursement: expenses sharing and supply. J Health Econ. 1986;5(2):129–52. 10.1016/0167-6296(86)90002-0. - PubMed
LinkOut - more resources
Full Text Sources
