

Sex-specific and metabolic subgroup heterogeneity in high-density lipoprotein cholesterol associations with diabetic kidney disease risk: a retrospective cohort study
- PMID: 40483478
- PMCID: PMC12144804
- DOI: 10.1186/s12944-025-02632-4
Sex-specific and metabolic subgroup heterogeneity in high-density lipoprotein cholesterol associations with diabetic kidney disease risk: a retrospective cohort study
Abstract
Background: The role of high-density lipoprotein cholesterol (HDL-C) in diabetic kidney disease (DKD) remains controversial. This study aimed to delineate the subgroup-specific relationships between the two by exploring cumulative and threshold effects.
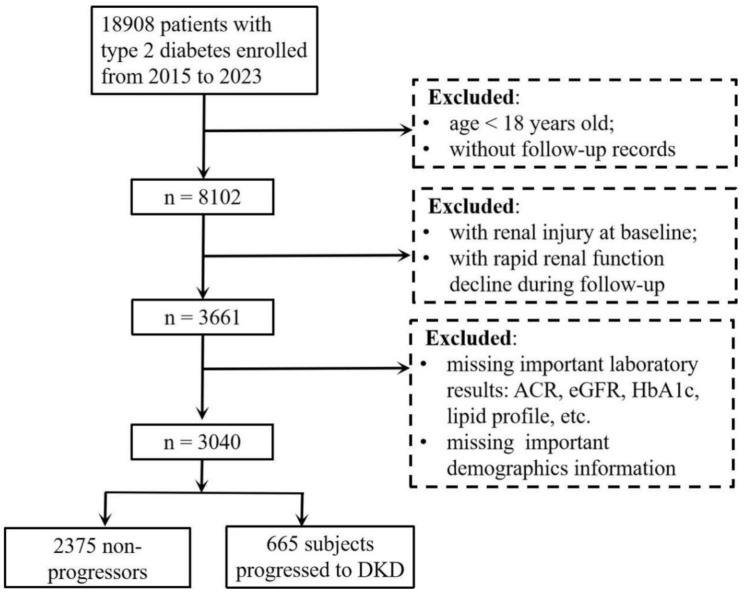
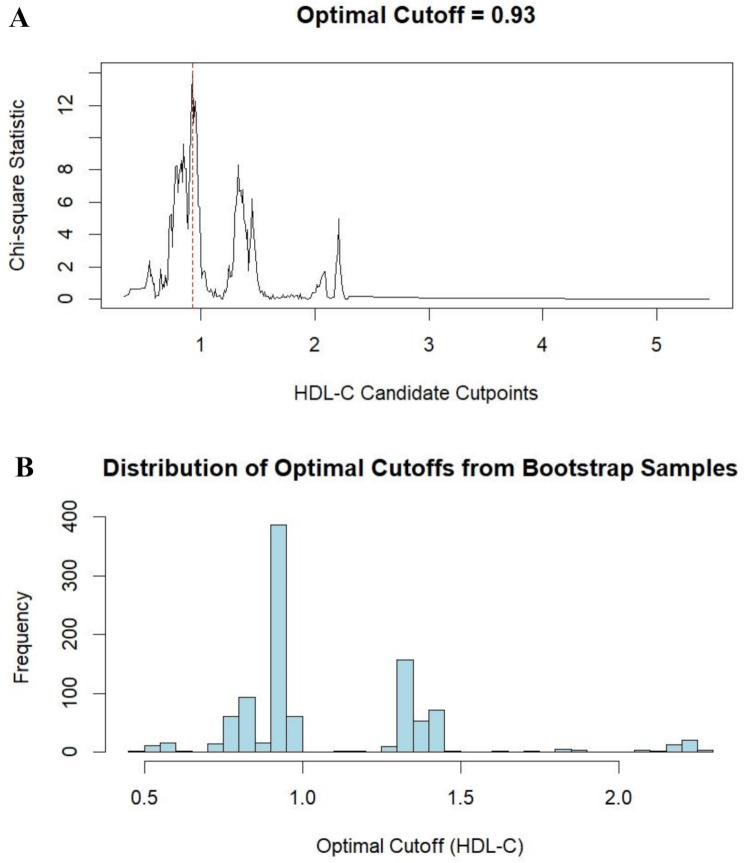
Methods: 3,040 patients with type 2 diabetes and no baseline evidence of DKD were included. Cox proportional hazards regression models were performed to investigate the potential relationship between HDL-C level and DKD risk. To address subgroup heterogeneity, sex-stratified restricted cubic splines (RCS) were employed to model nonlinear relationships. The optimal threshold was identified through the maximum selected statistics and validated via 1,000 bootstrap iterations. Subgroup analyses stratified by sex, diabetes duration, and metabolic status were performed to evaluate heterogeneity. Survival analysis using Kaplan-Meier curves further validated these threshold effects.
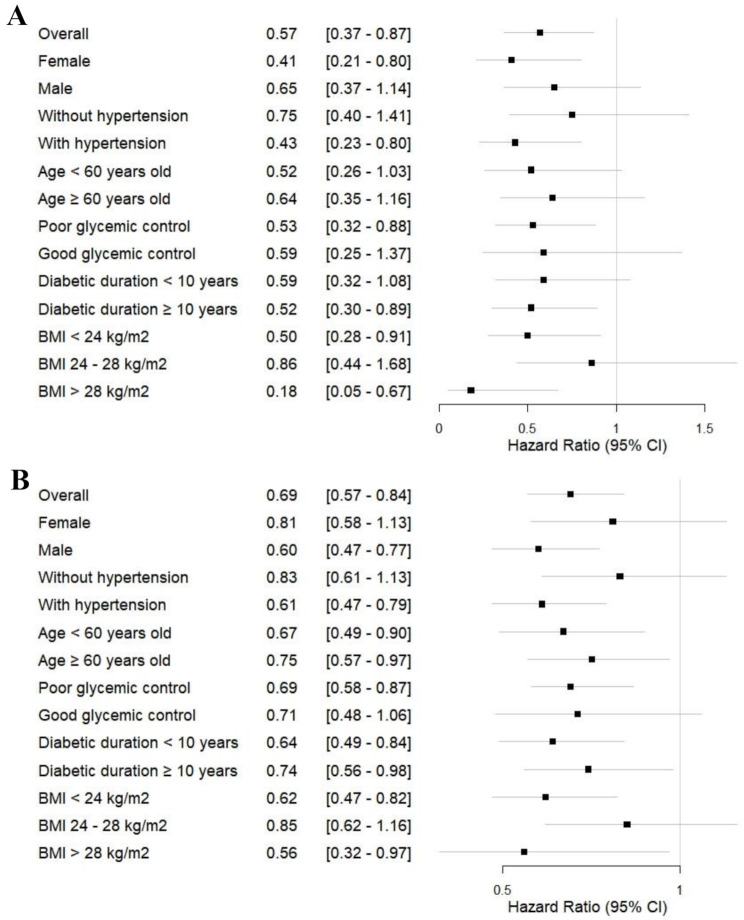
Results: During a median follow-up of 3.13 years, 665 subjects (21.9%) progressed to DKD. Overall, each 1 mmol/L increase in HDL-C level independently reduced DKD risk by 43%. RCS analysis demonstrated an inverse correlation between HDL-C and DKD risk (P for overall = 0.025, P for nonlinear = 0.317), with increased risk reduction at lower concentrations, plateauing at higher levels. A robust threshold of 0.93 mmol/L was identified, showing significantly stronger protection against DKD progression (hazard ratio (HR) = 0.69, P < 0.001) compared to the traditional cutoff (HR = 0.86, P = 0.109). Females showed continuous protection (HR = 0.41, P = 0.009) without threshold dependency. The male and diabetes duration < 10 years subgroups exhibited threshold effects at > 0.93 mmol/L without continuous protection. The metabolically unstable (hypertension, poorly controlled glycemia, body mass index (BMI) > 28 kg/m2) and BMI < 24 kg/m² subgroups displayed dual effects (P < 0.05). Survival analysis confirmed lower cumulative DKD incidence with HDL-C > 0.93 mmol/L (P = 0.007).
Conclusions: This study reveals sex- and metabolic context-dependent heterogeneity in HDL-C-DKD associations: males and short-duration diabetes exhibited threshold effects (0.93 mmol/L), females showed continuous protection, and subgroups with hypertension, poorly controlled glycemia, or obesity (BMI > 28 kg/m²) exhibited both continuous protection and threshold effects. These findings may inform individualized risk stratification in specific populations.
Keywords: Diabetic kidney disease; Dual effects; High-density lipoprotein cholesterol; Metabolic context-dependent; Subgroup heterogeneity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The present study followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Affiliated Jinhua Hospital, Zhejiang University School of Medicine (ethical approval number: (Res) 2024-Ethical Review-sb58). According to the regulations of the Ethics Committee, the consent for participation is not necessary for this retrospective study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
High levels of high-density lipoprotein cholesterol may increase the risk of diabetic kidney disease in patients with type 2 diabetes.Sci Rep. 2024 Jul 4;14(1):15362. doi: 10.1038/s41598-024-66548-2. Sci Rep. 2024. PMID: 38965304 Free PMC article.
-
Association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and cardiovascular disease mortality in patients with type 2 diabetes mellitus and diabetic kidney disease.Front Endocrinol (Lausanne). 2025 Feb 28;16:1509752. doi: 10.3389/fendo.2025.1509752. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40093754 Free PMC article.
-
Association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and diabetic kidney disease in patients with diabetes in the United States: a cross-sectional study.Lipids Health Dis. 2024 Sep 27;23(1):317. doi: 10.1186/s12944-024-02308-5. Lipids Health Dis. 2024. PMID: 39334123 Free PMC article.
-
High-Density Lipoprotein in Patients with Diabetic Kidney Disease: Friend or Foe?Int J Mol Sci. 2025 Feb 16;26(4):1683. doi: 10.3390/ijms26041683. Int J Mol Sci. 2025. PMID: 40004147 Free PMC article. Review.
-
Probiotics improve renal function, glucose, lipids, inflammation and oxidative stress in diabetic kidney disease: a systematic review and meta-analysis.Ren Fail. 2022 Dec;44(1):862-880. doi: 10.1080/0886022X.2022.2079522. Ren Fail. 2022. PMID: 35611435 Free PMC article.
Cited by
-
Gender-specific assessment of lipid profiles correlation with serum uric acid in non-dialysis chronic kidney disease patients: Prospective observational cross-sectional study.Front Endocrinol (Lausanne). 2025 Jul 30;16:1641978. doi: 10.3389/fendo.2025.1641978. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40810061 Free PMC article.
References
-
- Rayego-Mateos S, Rodrigues-Diez RR, Fernandez-Fernandez B, Mora-Fernández C, Marchant V, Donate-Correa J, Navarro-González JF, Ortiz A, Ruiz-Ortega M. Targeting inflammation to treat diabetic kidney disease: the road to 2030. Kidney Int. 2023;103(2):282–96. 10.1016/j.kint.2022.10.030 - PubMed
-
- Magliano DJ, Boyko EJ. DF diabetes atlas 10th edition scientific committee. IDF DIABETES ATLAS [Internet]. 10th ed. Brussels: International Diabetes Federation; 2021.
-
- Scilletta S, Di Marco M, Miano N, Filippello A, Di Mauro S, Scamporrino A, Musmeci M, Coppolino G, Di Giacomo Barbagallo F, Bosco G, Scicali R, Piro S, Purrello F, Di Pino A. Update on diabetic kidney disease (DKD): focus on Non-Albuminuric DKD and cardiovascular risk. Biomolecules. 2023;13(5):752. 10.3390/biom13050752 - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
