

Long-term multidimensional patient-centred outcomes after hospitalisation for COVID-19: do not only focus on disease severity
- PMID: 40484638
- PMCID: PMC12161316
- DOI: 10.1136/bmjresp-2024-002789
Long-term multidimensional patient-centred outcomes after hospitalisation for COVID-19: do not only focus on disease severity
Abstract
Objectives: To investigate the association between COVID-19 disease severity during hospitalisation for COVID-19 and long-term multidimensional patient-centred outcomes up to 12 months post-hospitalisation. The secondary objective was to identify other risk factors for these long-term outcomes.
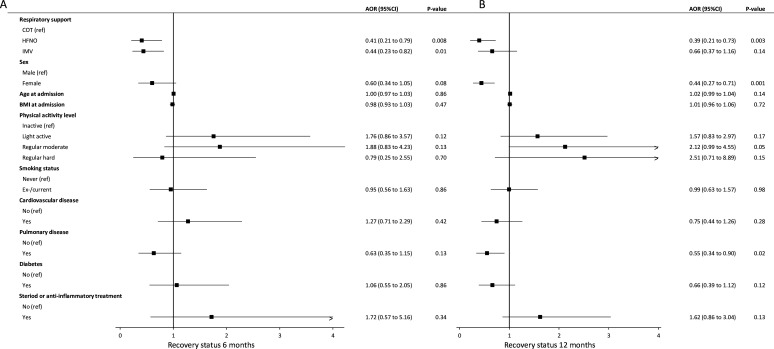
Methods: In this multicentre prospective cohort study, we categorised COVID-19 disease severity using the maximal level of respiratory support as proxy into (1) conventional oxygen therapy (COT), (2) high-flow nasal oxygen (HFNO) and (3) invasive mechanical ventilation (IMV). The primary outcome health-related quality of life (HRQoL), and the secondary outcomes self-reported symptoms and recovery were collected at 6 and 12 months post-hospitalisation.
Results: Data from 777 patients were analysed, with 226 (29%) receiving COT, 273 (35%) HFNO and 278 (36%) IMV. Patients reported impaired HRQoL, persistence of symptoms and poor recovery. Multivariable generalised estimating equations analysis showed that COVID-19 disease severity was not associated with HRQoL and inconsistently with symptoms; the HFNO group reported poorer recovery. Overall, female sex, younger age and pulmonary history were independent risk factors for outcomes.
Conclusions: COVID-19 disease severity was associated with self-perceived recovery, but not with HRQoL and inconsistently with symptoms. Our findings suggest that age, sex and pulmonary history are more consistent risk factors for long-term multidimensional outcomes and offer better guidance for aftercare strategies.
Keywords: COVID-19; Critical Care; Patient Outcome Assessment; Respiratory Infection.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: HE has received an unrestricted research grant from Fisher and Paykel Healthcare (Auckland, New Zealand) unrelated to this paper. The remaining authors have disclosed that they do not have any potential conflicts of interest related to this paper.
Figures



References
-
- Docherty AB, Mulholland RH, Lone NI, et al. Changes in in-hospital mortality in the first wave of COVID-19: a multicentre prospective observational cohort study using the WHO Clinical Characterisation Protocol UK. Lancet Respir Med. 2021;9:773–85. doi: 10.1016/S2213-2600(21)00175-2. - DOI - PMC - PubMed
-
- Hellemons ME, Huijts S, Bek LM, et al. Persistent Health Problems beyond Pulmonary Recovery up to 6 Months after Hospitalization for COVID-19: A Longitudinal Study of Respiratory, Physical, and Psychological Outcomes. Ann Am Thorac Soc. 2022;19:551–61. doi: 10.1513/AnnalsATS.202103-340OC. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous