

Real-world clinical outcomes in adult patients with Fabry disease: A 20-year retrospective observational cohort study from a single centre
- PMID: 40485669
- PMCID: PMC12144493
- DOI: 10.1016/j.ymgmr.2025.101229
Real-world clinical outcomes in adult patients with Fabry disease: A 20-year retrospective observational cohort study from a single centre
Abstract
Introduction: Fabry disease (FD) is an X-linked lysosomal storage disorder caused by alpha-galactosidase A deficiency, leading to the accumulation of globotriaosylceramide (Gb3) and progressive damage to the cardiovascular, renal, and cerebrovascular systems.
Aims: This study aimed to assess real-world clinical outcomes in FD patients, focusing on predominantly cardiovascular (CV), but also severe renal, and cerebrovascular outcomes, as well as CV and all-cause mortality. It also explored associations between age at diagnosis, Mainz Severity Score Index (MSSI), genetic mutations, and cardiometabolic risk factors such as smoking, hypertension, and obesity.
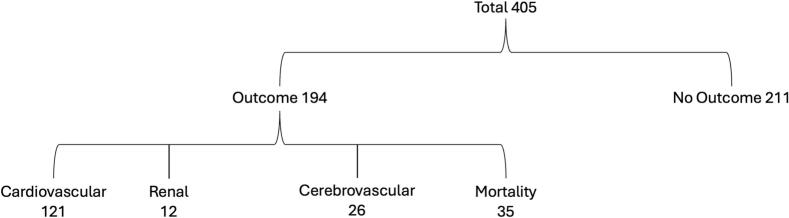
Methods: A retrospective observational cohort study of 405 patients with FD was conducted by reviewing medical records from a National Centre over a 20-year period. Clinical outcomes, predominantly cardiovascular, but also severe renal and cerebrovascular events and mortality were assessed. Age at diagnosis, MSSI, and cardiometabolic risk factors were also evaluated. Statistical comparisons were performed using the Mann-Whitney U test and Chi-square test, with significance set at p < 0.05.
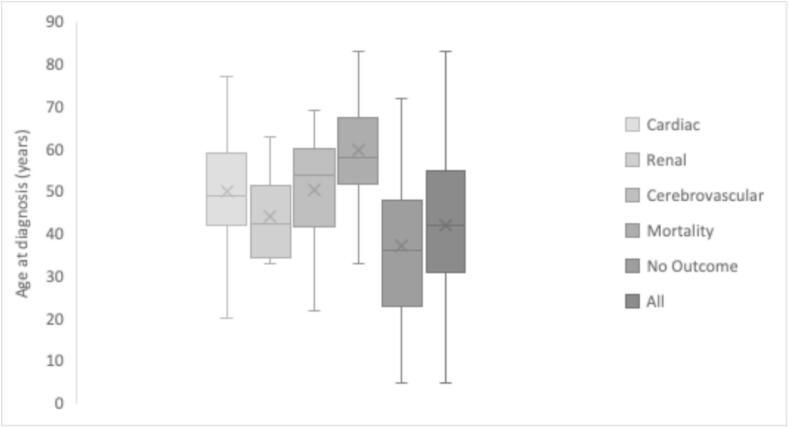
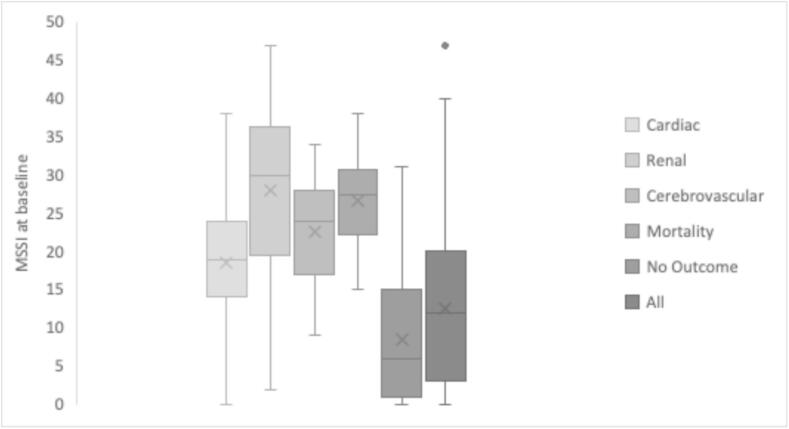
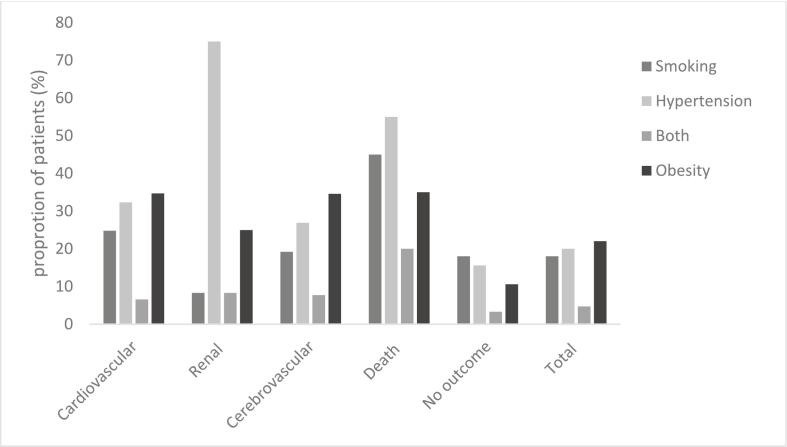
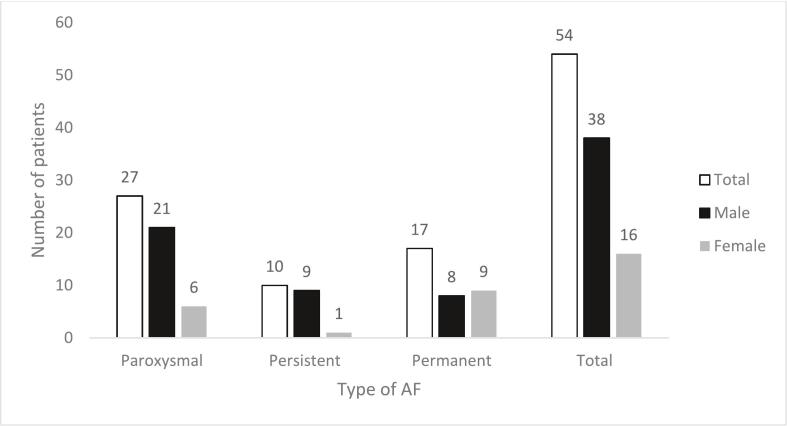
Results: Nearly half (48 %) of patients experienced a defined clinical outcome. Higher age at diagnosis and baseline MSSI was observed in patients with poorer outcomes. The c.644 A > G (p.N215S) variant was linked with increased cardiovascular morbidity and mortality. Cardiometabolic risk factors such as smoking, hypertension, and obesity were common in patients with poorer outcomes. A high prevalence of arrhythmia, including paroxysmal atrial fibrillation (AF), was observed. Multi-morbidity was noted in deceased patients. Use of cardiometabolic therapies in at-risk groups (e.g. sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists) was low.
Conclusion: This study highlights the clinical burden of FD, particularly among males with the c.644 A > G (p.N215S) variant. The frequent presence of cardiometabolic risk factors in patients with adverse outcomes reinforces the importance of early diagnosis, comprehensive risk evaluation, and individualised management to improve long-term prognosis.
Keywords: Alpha-galactosidase; Atrial fibrillation; Cardiometabolic; Fabry disease; Mainz severity score index (MSSI).
© 2025 The Authors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Phenotype and biochemical heterogeneity in late onset Fabry disease defined by N215S mutation.PLoS One. 2018 Apr 5;13(4):e0193550. doi: 10.1371/journal.pone.0193550. eCollection 2018. PLoS One. 2018. PMID: 29621274 Free PMC article.
-
Anderson-Fabry disease: a multiorgan disease.Curr Pharm Des. 2013;19(33):5974-96. doi: 10.2174/13816128113199990352. Curr Pharm Des. 2013. PMID: 23448451 Review.
-
Potential Usefulness of Lifetime Globotriaosylsphingosine Exposure at Diagnosis and Baseline Modified Disease Severity Score in Early-Diagnosed Patients With Fabry Disease.Cureus. 2024 May 30;16(5):e61380. doi: 10.7759/cureus.61380. eCollection 2024 May. Cureus. 2024. PMID: 38947680 Free PMC article.
-
Globotriaosylsphingosine (Lyso-Gb3) as a biomarker for cardiac variant (N215S) Fabry disease.J Inherit Metab Dis. 2018 Mar;41(2):239-247. doi: 10.1007/s10545-017-0127-2. Epub 2018 Jan 2. J Inherit Metab Dis. 2018. PMID: 29294190
-
Fabry Disease.2002 Aug 5 [updated 2024 Apr 11]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2002 Aug 5 [updated 2024 Apr 11]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301469 Free Books & Documents. Review.
References
LinkOut - more resources
Full Text Sources
