

Multicenter evaluation of the Quantra with the QStat Cartridge in adult trauma patients
- PMID: 40486089
- PMCID: PMC12142034
- DOI: 10.1136/tsaco-2024-001672
Multicenter evaluation of the Quantra with the QStat Cartridge in adult trauma patients
Abstract
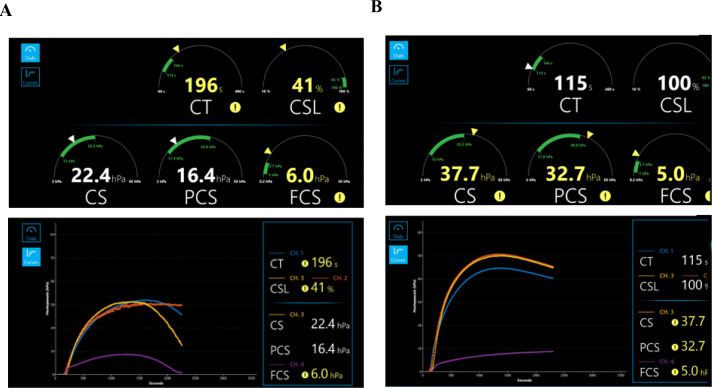
Background: Trauma-induced coagulopathy (TIC) occurs in a quarter of trauma patients and is associated with death due to uncontrolled bleeding. Current guidelines recommend viscoelastic testing (VET) to assess coagulopathy and guide transfusions. The Quantra with the QStat Cartridge is a point-of-care (POC) VET device that measures changes in clot stiffness (CS) during coagulation and fibrinolysis using ultrasound detection of resonance. This study aimed to evaluate the performance of the QStat Cartridge in trauma patients compared with rotational thromboelastometry (ROTEM) delta and thromboelastography (TEG) 6s VET devices.
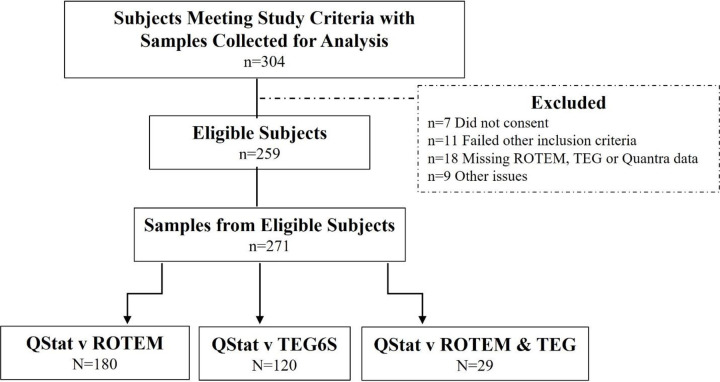
Methods: A multicenter prospective observational study was conducted in adult patients meeting criteria for a full trauma team response at eight US level 1 trauma centers. Citrated blood samples drawn on arrival at the hospital or after blood transfusions were analyzed in parallel on QStat, ROTEM or TEG. Correlation between QStat and equivalent VET measurements was assessed by linear regression. Concordance was assessed by agreement of results relative to device-specific normal reference ranges.
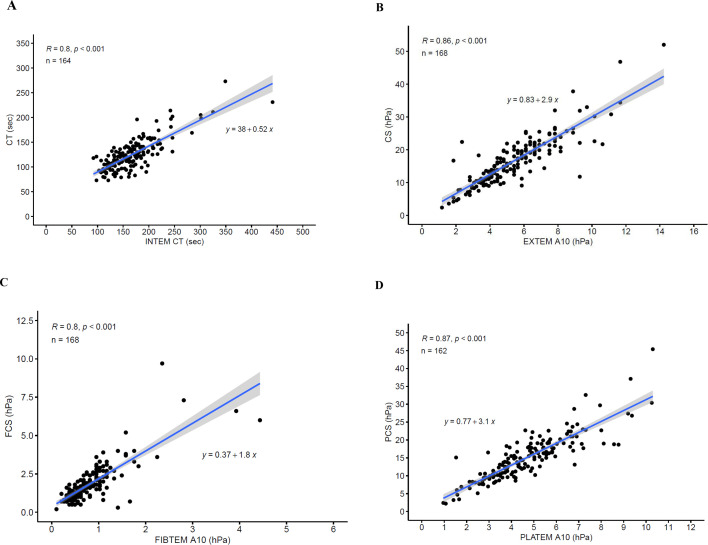
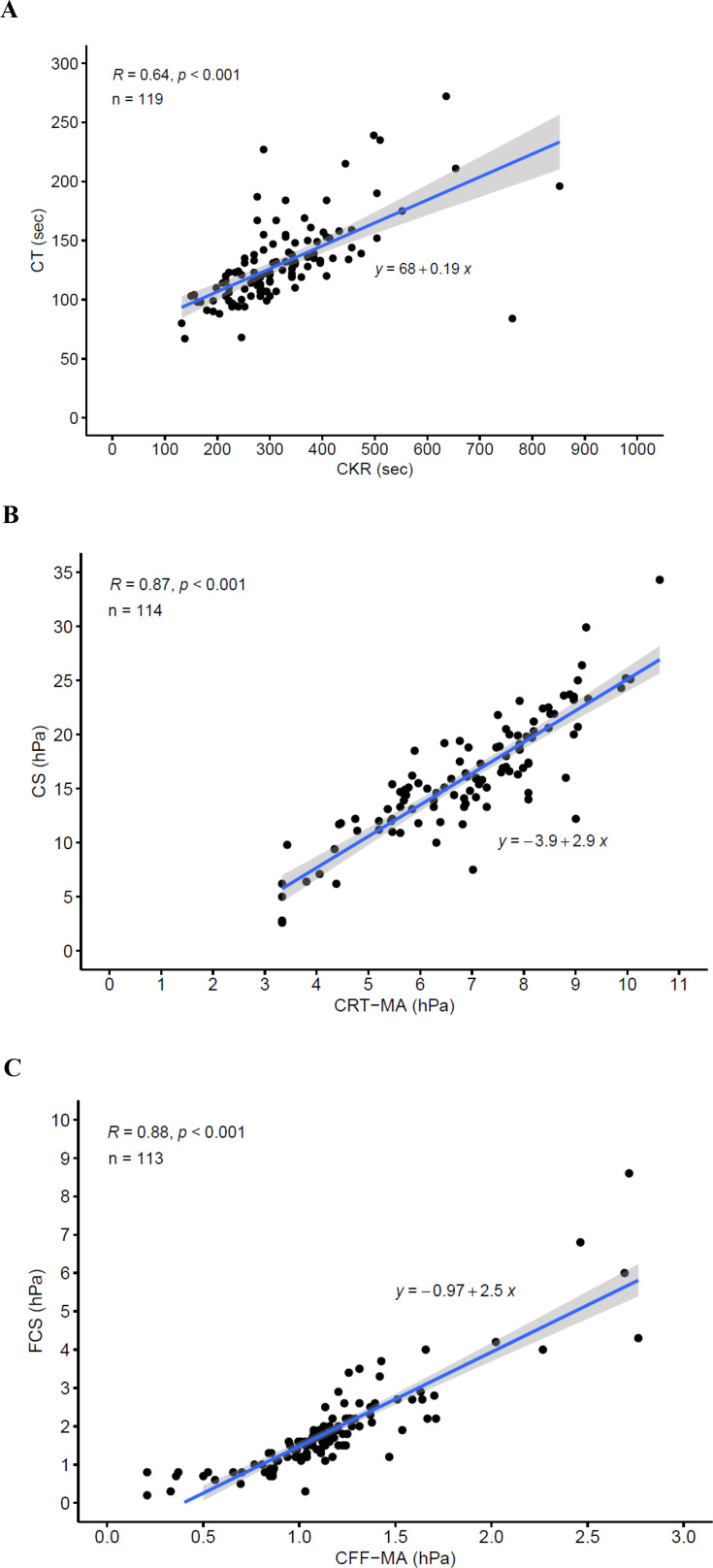
Results: 259 severely injured patients were enrolled, yielding 271 samples for analysis. Moderate to strong correlations between QStat and corresponding ROTEM and TEG measurements were observed (r=0.64-0.88). The concordance between CS results was 84.5% for QStat CS and EXTEM A10 and 83.3% for CS and citrated rapid TEG maximum amplitude. For fibrinogen-related results, concordance was 81.5% for QStat fibrinogen contribution to clot stiffness (FCS) and FIBTEM A10 and 93.8% for FCS and citrated functional fibrinogen maximum amplitude. For fibrinolysis measurements, the overall agreement between QStat clot stability to lysis and EXTEM ML or CK-LY30 was 97.5% and 92.9%, respectively.
Conclusion: QStat provides comparable information to the ROTEM delta and TEG 6s in trauma patients and can be useful for diagnosing TIC and guiding treatment. The Quantra's simplicity of use, ability to deploy at the POC, and rapid availability of results may provide clinicians with a faster, more convenient means to assess and manage TIC.
Level of evidence: Diagnostic test, level II.
Trial registration number: NCT04312958.
Keywords: blood coagulation tests; fibrinolysis; hemorrhage.
Copyright © Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
All institutions received research support from HemoSonics, LLC, for conduct of the study. In addition, EEM receives research support from Haemonetics, Humacyte and Prytime, and serves on a DSMB for Kcentra. EAM received an honorarium for a lecture from HemoSonics, LLC. MWC receives institutional support from Octapharma, serves on an advisory board for Grifols, and receives stock options from TraumaCare.AI, Inc. AF is a paid consultant for Werfen. KV receives research funding from Timewell Medical Co., Octapharma, and CELLPHIRE, and grant funding from SCA. FV and DAW are full-time employees of HemoSonics, LLC.
Figures
Comment in
-
Viscoelastic testing in trauma: not all that glitters is a gold standard.Trauma Surg Acute Care Open. 2025 Jun 8;10(2):e001919. doi: 10.1136/tsaco-2025-001919. eCollection 2025. Trauma Surg Acute Care Open. 2025. PMID: 40510862 Free PMC article. No abstract available.
References
-
- Rossaint R, Afshari A, Bouillon B, Cerny V, Cimpoesu D, Curry N, Duranteau J, Filipescu D, Grottke O, Grønlykke L, et al. The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition. Crit Care. 2023;27:80. doi: 10.1186/s13054-023-04327-7. - DOI - PMC - PubMed
-
- Gonzalez E, Moore EE, Moore HB, Chapman MP, Chin TL, Ghasabyan A, Wohlauer MV, Barnett CC, Bensard DD, Biffl WL, et al. Goal-directed Hemostatic Resuscitation of Trauma-induced Coagulopathy: A Pragmatic Randomized Clinical Trial Comparing a Viscoelastic Assay to Conventional Coagulation Assays. Ann Surg. 2016;263:1051–9. doi: 10.1097/SLA.0000000000001608. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials