

Artificial intelligence in resuscitation: a scoping review
- PMID: 40486106
- PMCID: PMC12142326
- DOI: 10.1016/j.resplu.2025.100973
Artificial intelligence in resuscitation: a scoping review
Abstract
Background: Artificial intelligence (AI) is increasingly applied in medicine, with growing interest in its potential to improve outcomes in cardiac arrest (CA). However, the scope and characteristics of current AI applications in resuscitation remain unclear.
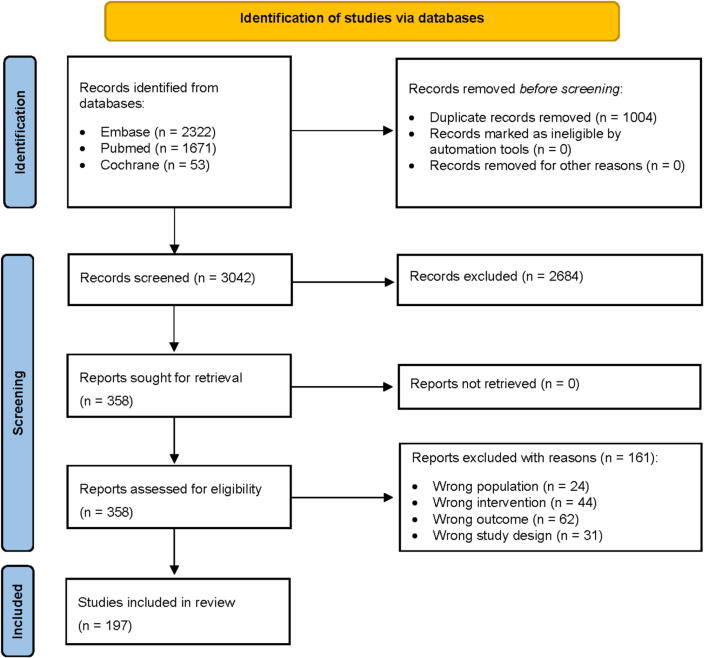
Methods: This scoping review aims to map the existing literature on AI applications in CA and resuscitation and identify research gaps for further investigation. PRISMA-ScR framework and ILCOR guidelines were followed. A systematic literature search across PubMed, EMBASE, and Cochrane identified AI applications in resuscitation. Articles were screened and classified by AI methodology, study design, outcomes, and implementation settings. AI-assisted data extraction was manually validated for accuracy.
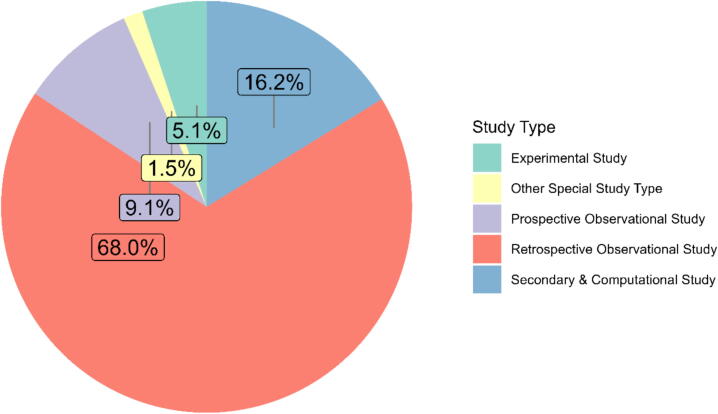
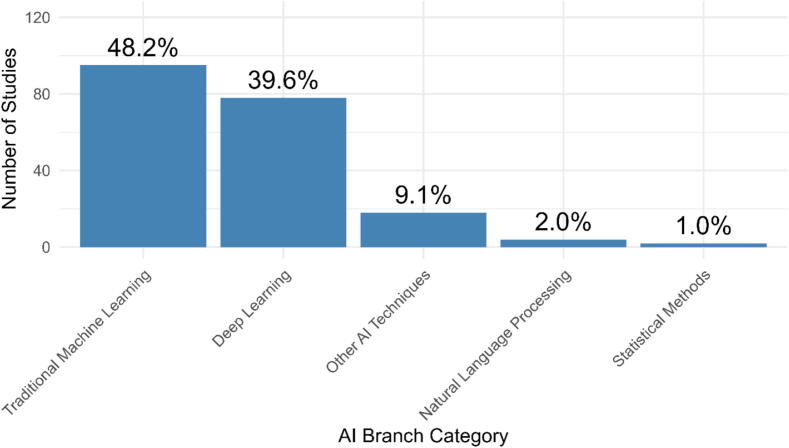
Results: Out of 4046 records, 197 studies met inclusion criteria. Most were retrospective (90%), with only 16 prospective studies and 2 randomised controlled trials. AI was predominantly applied in prediction of CA, rhythm classification, and post-resuscitation outcome prognostication. Machine learning was the most commonly used method (50% of studies), followed by deep learning and, less frequently, natural language processing. Reported performance was generally high, with AUROC values often exceeding 0.85; however, external validation was rare and real-world implementation limited.
Conclusions: While AI applications in resuscitation demonstrate encouraging performance in prediction and decision support tasks, clear evidence of improved patient outcomes or routine clinical use remains limited. Future research should focus on prospective validation, equity in data sources, explainability, and seamless integration of AI tools into clinical workflows.
Keywords: Artificial intelligence; Cardiac arrest; Deep learning; Large language model; Machine learning; Resuscitation; Scoping review.
© 2025 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: FS is the Chair of the European Resuscitation Council, an Emeritus member of the ILCOR BLS Working Group, and a member of the Italian Resuscitation Council Foundation, SS is an ILCOR EIT Task Force member, ERC Advanced Life Support Science and Education Committee member, and Vice Chair of the Austrian Resuscitation Council, JM is a co-founder and shareholder of Callisia srl University Spin-off at Università Politecnica delle Marche developing a smart bracelet collecting patient data intelligently for real-time visualization and data analysis, GR is the Director of Congresses for the European Resuscitation Council, an Emeritus member of the ILCOR BLS Working Group, member of the Italian Resuscitation Council Foundation and Resuscitation Plus Editorial board member. NF Fijačko is a member of the ERC BLS Science and Education Committee, LG is a member of the Scientific Committee of the Italian Resuscitation Council, EGB is the Chair of SIAARTI Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care, RG is ERC Director of Guidelines and ILCOR, ILCOR Task Force chair for Education Implementation and Team and Resuscitation Plus Editorial board member. AS is the President of the Italian Resuscitation Council. KGM, DZ has no conflict of interest.
Figures
Similar articles
-
Artificial intelligence for breast cancer detection and its health technology assessment: A scoping review.Comput Biol Med. 2025 Jan;184:109391. doi: 10.1016/j.compbiomed.2024.109391. Epub 2024 Nov 22. Comput Biol Med. 2025. PMID: 39579663
-
Applying AI to Structured Real-World Data for Pharmacovigilance Purposes: Scoping Review.J Med Internet Res. 2024 Dec 30;26:e57824. doi: 10.2196/57824. J Med Internet Res. 2024. PMID: 39753222 Free PMC article.
-
Application of Artificial Intelligence in Community-Based Primary Health Care: Systematic Scoping Review and Critical Appraisal.J Med Internet Res. 2021 Sep 3;23(9):e29839. doi: 10.2196/29839. J Med Internet Res. 2021. PMID: 34477556 Free PMC article.
-
The Role of Artificial Intelligence Model Documentation in Translational Science: Scoping Review.Interact J Med Res. 2023 Jul 14;12:e45903. doi: 10.2196/45903. Interact J Med Res. 2023. PMID: 37450330 Free PMC article.
-
Artificial Intelligence in Thoracic Surgery: A Review Bridging Innovation and Clinical Practice for the Next Generation of Surgical Care.J Clin Med. 2025 Apr 16;14(8):2729. doi: 10.3390/jcm14082729. J Clin Med. 2025. PMID: 40283559 Free PMC article. Review.
Cited by
-
Optimization of dispatcher instruction for public-access automated external defibrillator retrieval and use: A scoping review.Resusc Plus. 2025 Jun 14;25:101005. doi: 10.1016/j.resplu.2025.101005. eCollection 2025 Sep. Resusc Plus. 2025. PMID: 40636079 Free PMC article. Review.
-
Artificial intelligence as a virtual dispatcher: Decision support for lay responders in simulated cardiac arrest scenarios.Resusc Plus. 2025 Jul 25;25:101043. doi: 10.1016/j.resplu.2025.101043. eCollection 2025 Sep. Resusc Plus. 2025. PMID: 40791935 Free PMC article. No abstract available.
References
-
- Perkins GD, Graesner JT, Semeraro F, et al. European Resuscitation Council Guideline Collaborators. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation. 2021;161:1–60. 10.1016/j.resuscitation.2021.02.003. Epub 2021 Mar 24. Erratum in: Resuscitation. 2021 May 4;163:97-98. doi: 10.1016/j.resuscitation.2021.04.012.. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
