

The impact of renin-angiotensin system inhibitors on colorectal neoplasm development
- PMID: 40486129
- PMCID: PMC12145888
- DOI: 10.5646/ch.2025.31.e22
The impact of renin-angiotensin system inhibitors on colorectal neoplasm development
Abstract
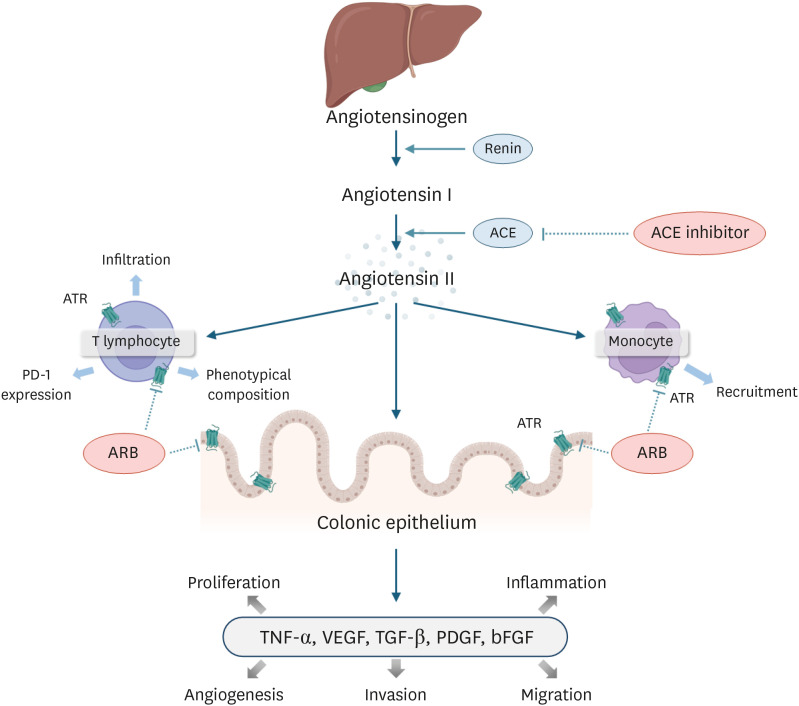
Background: Renin-angiotensin system (RAS) inhibitors have shown potential chemopreventive effects against colorectal cancer (CRC). However, little is known about the impact of RAS inhibitors on the risk of colorectal precancerous lesions.
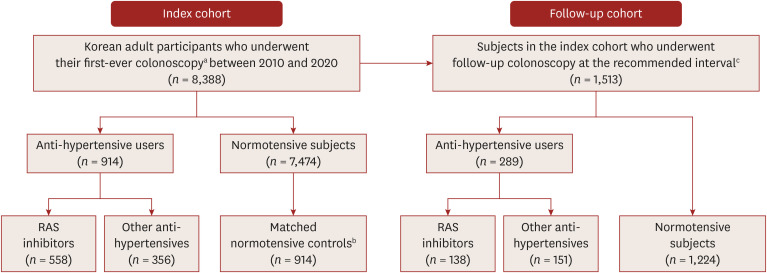
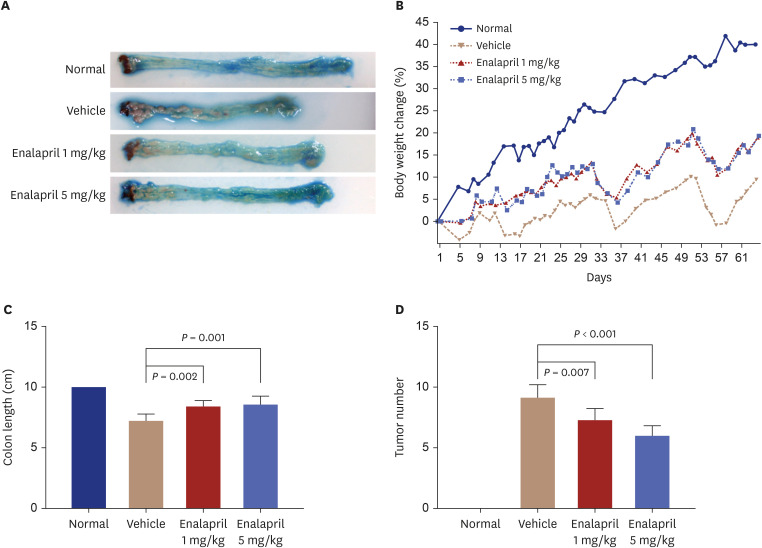
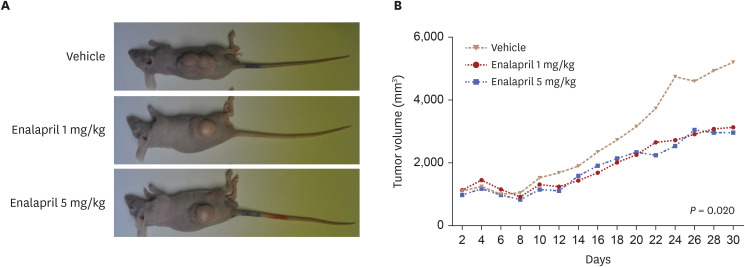
Methods: Preclinically, we established mouse models of colitis-associated colon cancer and xenografts: vehicle, 1 mg/kg, 5 mg/kg enalapril groups. Body weight, colon length, and colorectal tumor size were evaluated on the euthanization day. Clinically, we retrospectively recruited 8,388 asymptomatic adults undergoing their first-ever colonoscopy for health check-ups (index cohort). From the index cohort, we selected individuals undergoing follow-up colonoscopy (follow-up cohort). The study outcome was incidental and recurrent colorectal neoplasms, including CRC. We evaluated the prevalence and risk of colorectal neoplasms associated with RAS inhibitor use of ≥ 1 year.
Results: In the experimental study, enalapril administration significantly attenuated weight loss and colon shortening, reduced tumor numbers in colitis-associated colon cancer models, and decreased tumor volume in the xenografts. In the index cohort, while the initial analysis showed a positive association with the RAS inhibitor use (unadjusted odds ratio [OR], 1.22), this shifted toward an inverse trend after adjusting for confounders (adjusted OR, 0.91). During follow-up (median, 41.0 months), incidental and recurrent colorectal neoplasms were less common in the RAS inhibitor group (32.6%) than in the other anti-hypertensives group (39.1%) (P < 0.001), despite similar intervals between the index and follow-up endoscopies. In the follow-up cohort, hypertension itself was a risk factor for colorectal neoplasm development (adjusted hazard ratio [HR], 1.70; 95% confidence interval [CI], 1.00-2.53; P = 0.049), whereas RAS inhibitor use was significantly associated with a 27% lower risk (adjusted HR, 0.73; 95% CI, 0.59-0.95; P = 0.035).
Conclusions: Long-term, regular use of RAS inhibitors independently reduces the risk of colorectal neoplasms, irrespective of dosage or drug type. Given their potential chemopreventive effects on colorectal neoplasms, RAS inhibitors may serve as a preventive strategy starting from the precancerous stage.
Keywords: Chemoprevention; Colorectal cancer; RAS inhibitor; Translational research.
Copyright © 2025 The Korean Society of Hypertension.
Conflict of interest statement
Competing interest: The authors declare that they have no competing interests.
Figures
Comment in
-
RAS inhibitors and their translational relevance in colorectal neoplasia.Clin Hypertens. 2025 Oct 1;31:e29. doi: 10.5646/ch.2025.31.e29. eCollection 2025. Clin Hypertens. 2025. PMID: 41089591 Free PMC article. No abstract available.
References
-
- Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24:2137–2150. - PubMed
-
- Araghi M, Soerjomataram I, Jenkins M, Brierley J, Morris E, Bray F, et al. Global trends in colorectal cancer mortality: projections to the year 2035. Int J Cancer. 2019;144:2992–3000. - PubMed
-
- National Cancer Information Center. 2020. [Accessed 6 Dec 2024]. https://www.cancer.go.kr/index.do .
-
- Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, et al. Global cancer observatory: cancer today. [Accessed 6 Dec 2024]. https://gco.iarc.fr/today .
-
- Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, et al. Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19:329–359. - PubMed
LinkOut - more resources
Full Text Sources