

Altered liver sinusoidal endothelial cells in MASLD and their evolution following lanifibranor treatment
- PMID: 40486133
- PMCID: PMC12142333
- DOI: 10.1016/j.jhepr.2025.101366
Altered liver sinusoidal endothelial cells in MASLD and their evolution following lanifibranor treatment
Abstract
Background & aims: Data on changes in liver sinusoidal endothelial cells (LSECs) in patients with metabolic dysfunction-associated steatotic liver disease (MASLD) and their response to treatment are limited. This study aimed at determining (i) features associated with LSEC capillarisation in patients with MASLD; (ii) whether LSEC changes can regress with the pan-peroxisome proliferator-activated receptor (PPAR) agonist lanifibranor; (iii) the role of the different PPAR isotypes on LSEC changes in MASLD.
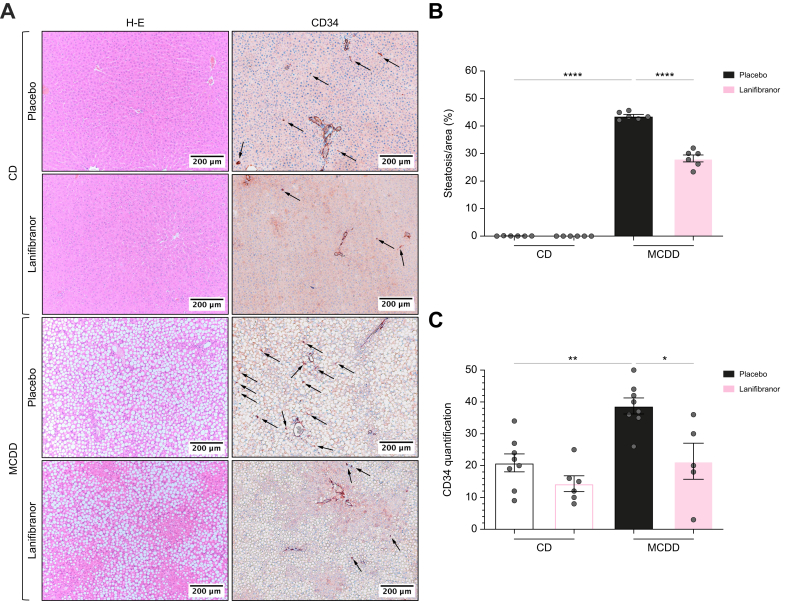
Methods: We analysed CD34 expression, a marker of LSEC capillarisation, on liver biopsies from patients considered for inclusion in the NATIVE trial at baseline (n = 249), and after 24 weeks of placebo or lanifibranor (n = 173). Two rat models of MASLD were used to investigate the effect of lanifibranor or of mono-PPAR agonists on LSECs.
Results: Lobular CD34 staining was more intense in patients with isolated steatosis than in those with no MASLD (52% vs. 10%; p = 0.03). In the overall cohort, this staining was more intense in patients with metabolic dysfunction-associated steatohepatitis (MASH) than in those without (63% vs. 41%; p = 0.01) and strongly correlated with liver fibrosis and to a lesser extent with liver inflammation. Lanifibranor treatment was associated with more common improvement in CD34 periportal staining (p = 0.025), and less frequent worsening of lobular staining (p = 0.028). Compared with healthy rats, rats with MASLD had higher CD34 staining, portal venous pressure, intrahepatic vascular resistance, and impaired liver endothelial function. Lanifibranor normalised or strongly improved these abnormalities, whereas mono-PPAR agonists caused partial improvements.
Conclusions: In patients, LSEC capillarisation was increased at the earliest stages of MASLD and was associated with liver fibrosis and inflammation. In both patients and rats with MASLD, lanifibranor treatment was associated with improvement in liver endothelial phenotype.
Impact and implications: Data on changes in liver sinusoidal endothelial cells (LSECs) in patients with metabolic dysfunction-associated steatotic liver disease (MASLD) and their response to treatment are limited. This study demonstrates that LSEC capillarisation is already present in the lobular zone of the liver of patients and rats at the stage of isolated steatosis, before metabolic dysfunction-associated steatohepatitis (MASH) onset, and progresses with liver fibrosis, and to a lesser extent with liver inflammation. Lanifibranor treatment, a pan-peroxisome proliferator-activated receptor agonist currently tested in a phase III clinical trial, improves LSEC capillarisation but also intrahepatic vascular resistance and portal pressure in MASLD. Targeting LSECs appears to be a promising approach to improve MASH.
Keywords: CD34; Intrahepatic vascular resistance; LSECs; Liver fibrosis; Liver inflammation; MASH; PPAR; Vascular biology; lanifibranor.
© 2025 The Authors.
Conflict of interest statement
P-ER has received research funding from Terrafirma and acted as consultant for Mursla, Genfit, Boehringer Ingelheim, Cook, Jazz, and Abbelight, and received speaker fees from AbbVie. SMF has been lecturer for AbbVie, Allergan, Bayer, Eisai, Genfit, Gilead Sciences, Janssens Cilag, Intercept, Inventiva, Merck Sharp & Dome, Novo Nordisk, Promethera, Siemens. He has acted as consultant for AbbVie, Actelion, Aelin Therapeutics, AgomAb, Aligos Therapeutics, Allergan, Astellas, Astra Zeneca, Bayer, Boehringer Ingelheim, Bristoll-Meyers Squibb, CSL Behring, Coherus, Echosens, Eisai, Enyo, Galapagos, Galmed, Genetech, Genfit, Genflow Bio, Gilead Sciences, Intercept, Inventiva, Janssens Pharmaceutica, Julius Clinical, Madrigal, Medimmune, Merck Sharp & Dome, NGM Bio, Novartis, Novo Nordisk, PRO.MED.CS, Promethera, Roche. His institution has received grants from Astellas, Falk Pharma, Genfit, Gilead Sciences, GlympsBio, Janssens Pharmaceutica, Inventiva, Merck Sharp & Dome, Pfizer, Roche. WJK received lecturer fees for the PanNASH initiative and received travel grants from Ipsen and Norgine. He is a co-inventor of a patent on the use of lipopigment imaging for disease (filed by MGH/MIT: US 20190307390). MFA has acted as an advisor for 89Bio, Boehringer Ingelheim, Hanmi, Intercept, Inventiva, Madrigal, and Novo Nordisk. She has received grants (paid to her institution) from 89Bio, Akero, Hamni, Inventiva, Madrigal and Novo Nordisk. She has served as a speaker for MedScape, Chronic Liver Disease Foundation, Clinical Care Options, and Fishawack, Inc. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures







References
-
- Rinella M.E., Lazarus J.V., Ratziu V., et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79:1542–1556. - PubMed
-
- EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64:1388–1402. - PubMed
-
- Francque S., Szabo G., Abdelmalek M.F., et al. Nonalcoholic steatohepatitis: the role of peroxisome proliferator-activated receptors. Nat Rev Gastroenterol Hepatol. 2021;18:24–39. - PubMed
LinkOut - more resources
Full Text Sources
