

Uncommon but intriguing: A pediatric primary histiocytic sarcoma case-Clinical insights and literature review
- PMID: 40486162
- PMCID: PMC12144458
- DOI: 10.1016/j.radcr.2025.04.063
Uncommon but intriguing: A pediatric primary histiocytic sarcoma case-Clinical insights and literature review
Abstract
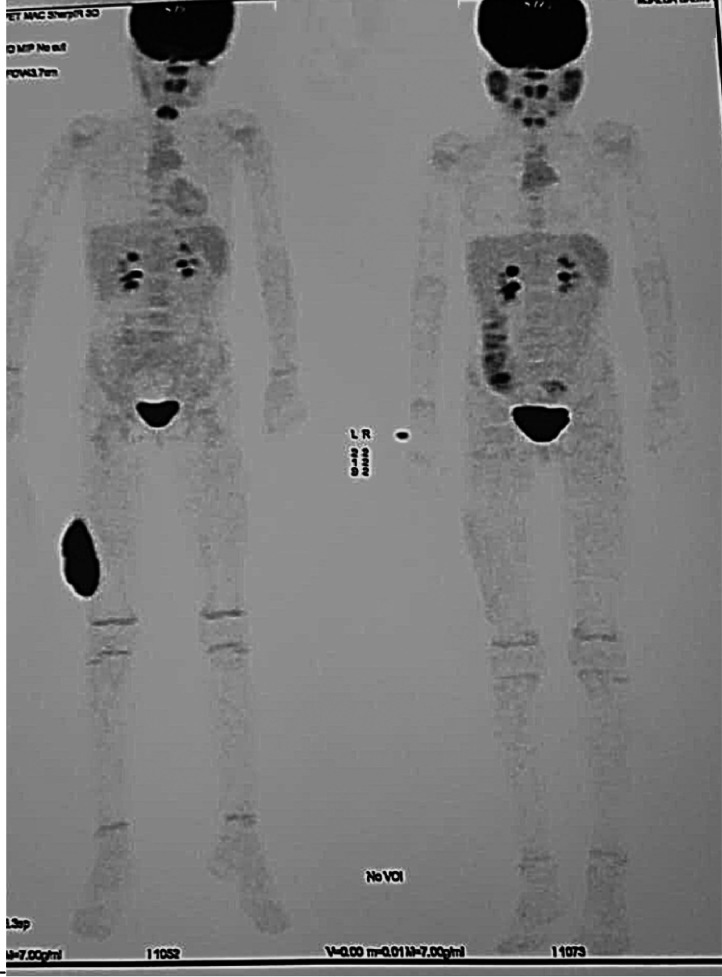
Histiocytic sarcoma (HS) is a rare and aggressive malignancy derived from histiocytes, accounting for less than 1% of hematopoietic neoplasms. Pediatric soft tissue involvement is exceptionally rare, with limited data to guide management. We present the case of a 5-year-old girl with a painless mass on the right thigh. Imaging revealed a malignant intra-aponeurotic soft tissue lesion. Histopathological analysis confirmed HS with immunohistochemical positivity for CD68, CD31, LCA, and INI1, and a Ki-67 index of 40%. Staging PET-CT identified local lymph node involvement. Following R1 surgical resection, the patient received adjuvant radiotherapy (43 Gy to the tumor bed and 36.9 Gy to the inguinal region) and OEPAbased chemotherapy. At 20 months post-treatment, the patient remains in remission with excellent functional outcomes. This case highlights the rarity of soft tissue histiocytic sarcoma in pediatric patients and the importance of multimodal treatment to achieve long-term remission.
Keywords: Histiocytic; Oncology; Pediatric cancer; Radiotherapy; Soft tissue sarcoma.
© 2025 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



References
-
- Pileri S.A., Grogan T.M., Harris N.L., Banks P., Campo E., Chan J.K., et al. Histiocytic sarcoma: clinicopathologic study of 21 cases. Blood. 2002;100(2):766–773.
-
- Takahashi E., Nakamura S. Histiocytic sarcoma: an updated literature review based on the 2008 WHO classification. J Clin Exp Hematopathol. 2013;53(1):1–8. - PubMed
-
- Hornick J.L., Jaffe E.S., Fletcher CD. Histiocytic sarcoma: A study of 14 cases with emphasis on morphologic heterogeneity. Am J Surg Pathol. 2004;28(6):697–704. - PubMed
-
- Cheng J., Zhu G., Pan M., Gong S., Mo J., Pan Z. Pediatric histiocytic disorders: morphology, immunophenotype and genetics. J Clin Transl Pathol. 2023;3(4):151–159. doi: 10.14218/JCTP.2023.00027. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
