

Comparative Effectiveness of High-Flow Nasal Cannula and Noninvasive Ventilation in Acute Hypoxemic Respiratory Failure: A Scoping Review
- PMID: 40486342
- PMCID: PMC12145221
- DOI: 10.7759/cureus.83752
Comparative Effectiveness of High-Flow Nasal Cannula and Noninvasive Ventilation in Acute Hypoxemic Respiratory Failure: A Scoping Review
Abstract
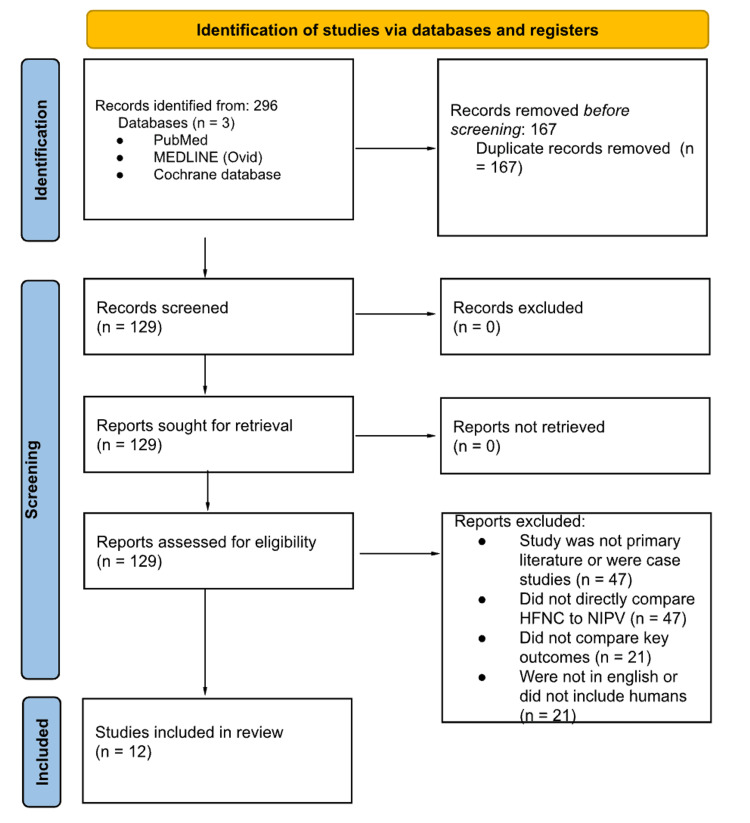
Acute hypoxemic respiratory failure (AHRF) is a leading cause of ICU admissions, and noninvasive respiratory support modalities such as high-flow nasal cannula (HFNC) and noninvasive ventilation (NIV) are frequently employed. However, the comparative effectiveness of these two interventions across different patient populations remains unclear. This scoping review aimed to synthesize current evidence comparing HFNC and NIV in the management of adult patients with AHRF, focusing on outcomes such as intubation rates, mortality, patient comfort, oxygenation, and complications. Studies were included if they: (1) were primary research articles, (2) involved human adults with AHRF, (3) directly compared HFNC with NIV, and (4) reported on clinical outcomes. Systematic reviews, case reports, editorials, and studies focused exclusively on immunocompromised or postoperative populations were excluded. A systematic search of PubMed, MEDLINE (via Ovid), and the Cochrane Library was conducted through February 2025. Three independent reviewers screened and selected studies using Rayyan. Data extraction was performed using a structured template capturing study design, sample size, population, intervention details, and relevant outcomes. Twelve studies met the inclusion criteria. HFNC and NIV demonstrated comparable effectiveness in reducing intubation rates across most patient populations. In COVID-19-associated AHRF, the two modalities yielded similar outcomes in terms of intubation and mortality. HFNC was consistently associated with greater patient comfort and fewer complications, particularly with respect to interface tolerance and skin breakdown. However, NIV remained more effective in clearing carbon dioxide, especially in patients with hypercapnic respiratory failure, such as those with COPD exacerbations. ORs were infrequently reported; however, one study reported an adjusted hazard ratio of 0.75 (95% CI: 0.58-0.98) favoring HFNC over oxygen masks for ICU mortality. HFNC may be preferable for patients who have difficulty tolerating masks or are at lower risk for hypercapnia, while NIV remains the standard of care in hypercapnic respiratory failure. Mortality outcomes were inconclusive. Future randomized controlled trials should target specific patient subgroups and examine long-term outcomes and hospital resource utilization to optimize noninvasive respiratory support strategies in AHRF.
Keywords: acute hypoxemic respiratory failure; copd exacerbation; covid-19; critical care; high-flow nasal cannula; intubation; mechanical ventilation avoidance; noninvasive ventilation; oxygen therapy; respiratory support.
Copyright © 2025, Kunder et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Epidemiology and outcome of acute respiratory failure in intensive care unit patients. Vincent JL, Sakr Y, Ranieri VM. Crit Care Med. 2003;31:0. - PubMed
-
- One-year outcomes in survivors of the acute respiratory distress syndrome. Herridge MS, Cheung AM, Tansey CM, et al. N Engl J Med. 2003;348:683–693. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous