

Successful Laparoscopic-Assisted Pancreaticoduodenectomy for a Neuroendocrine Tumor of the Papilla of Vater in Type 1 Portal Annular Pancreas
- PMID: 40487385
- PMCID: PMC12142215
- DOI: 10.70352/scrj.cr.25-0085
Successful Laparoscopic-Assisted Pancreaticoduodenectomy for a Neuroendocrine Tumor of the Papilla of Vater in Type 1 Portal Annular Pancreas
Abstract
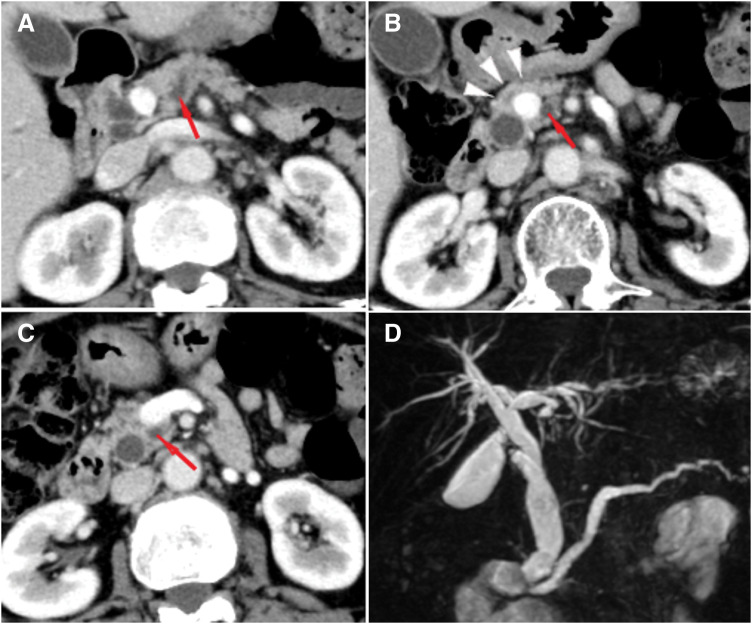
Introduction: Portal annular pancreas (PAP) is a rare anomaly of pancreatic embryology that is classified into three types according to the position of the main pancreatic duct. PAP type 1, in which the main pancreatic duct runs dorsal to the pancreas, is extremely rare. Herein, we describe a case of successful laparoscopic-assisted pancreaticoduodenectomy in a patient with type 1 PAP.
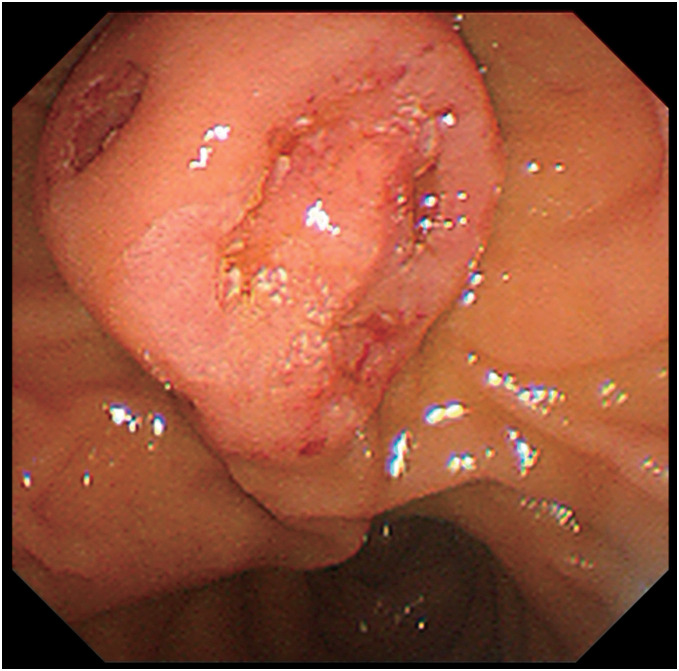
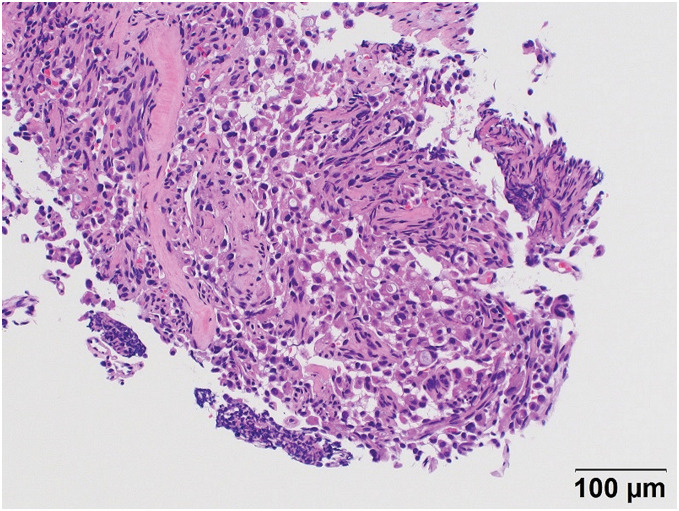
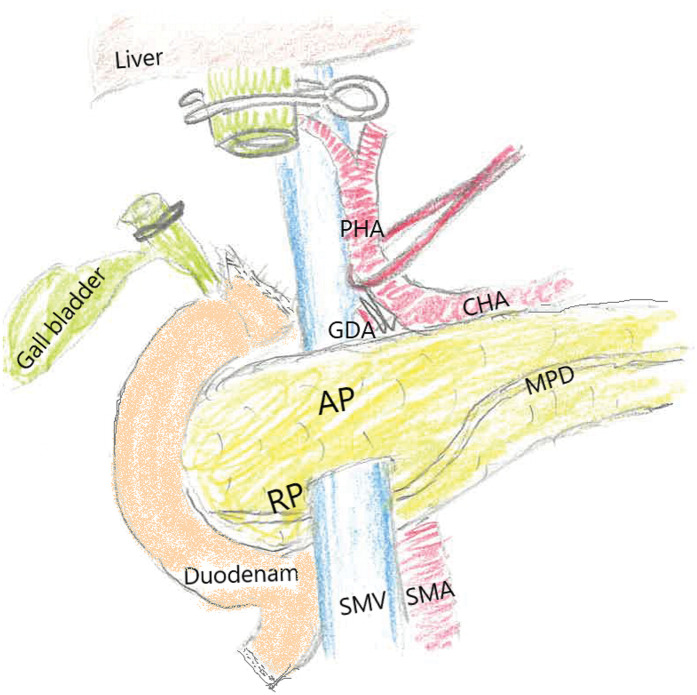
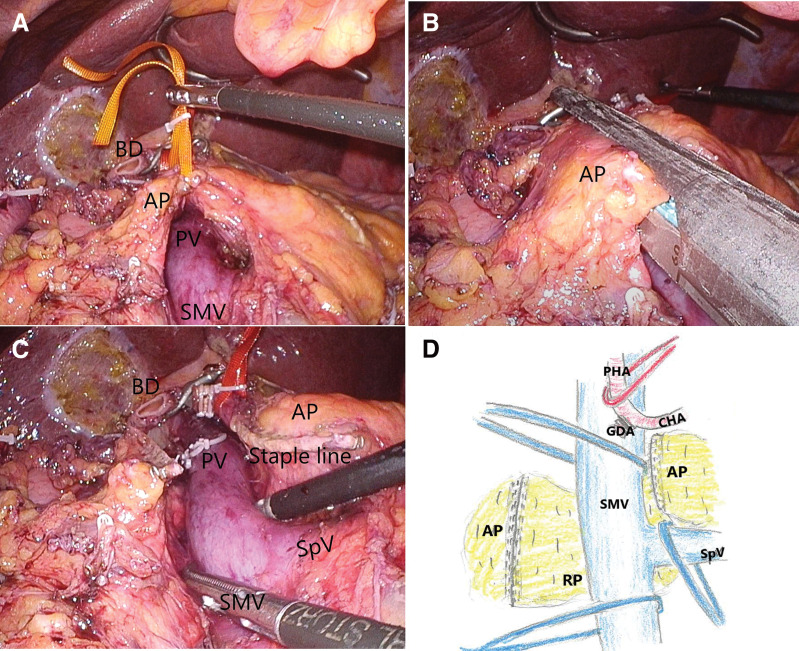
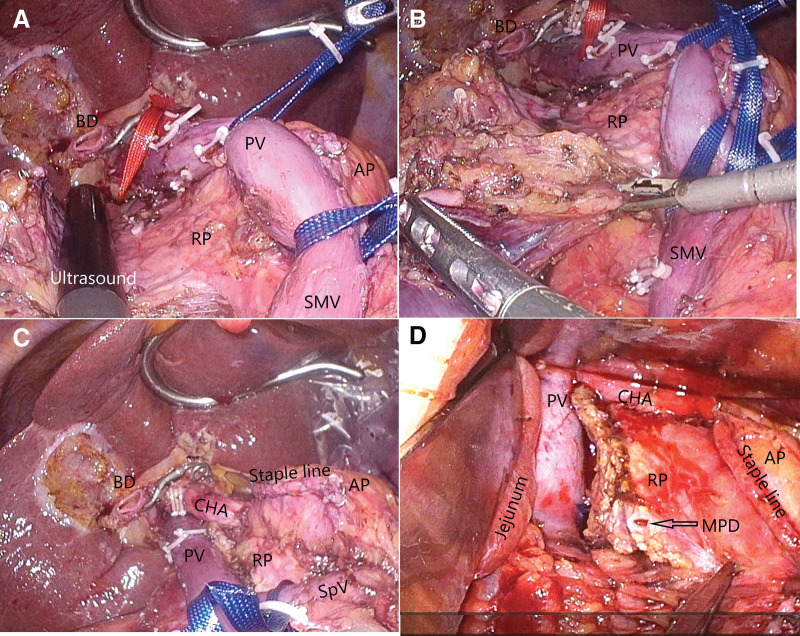
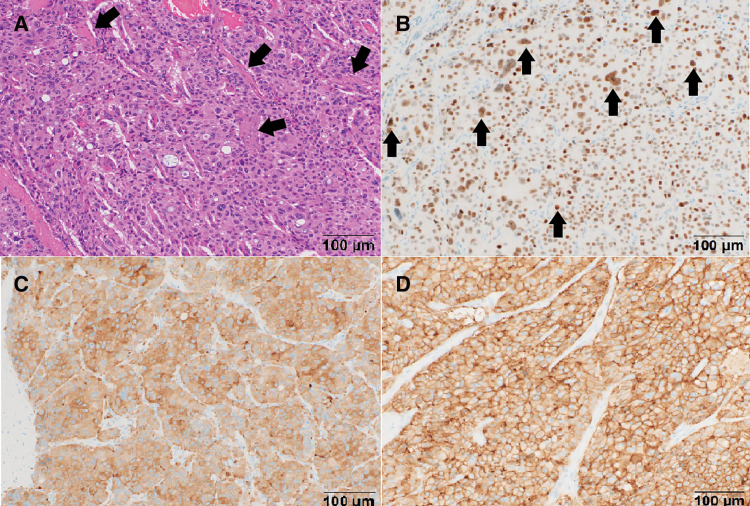
Case presentation: A 72-year-old Japanese woman with neck swelling was referred to our hospital. CT at admission showed dilation of the main pancreatic duct. After a thorough examination, a preoperative diagnosis of carcinoma of the papilla of Vater was made. Neck swelling was attributed to a lymphoma for which chemotherapy was administered. Upon remission, CT imaging indicated PAP type 1, and a laparoscopic-assisted pancreaticoduodenectomy was performed. The retroportal pancreas was dissected just below the portal vein, but anastomosis was difficult; therefore, the pancreas was moved to the anterior surface of the portal vein, and anastomosis was performed. Postoperative pancreatic leakage occurred but was relieved by drainage, and the patient was discharged 26 days postoperatively. The postoperative diagnosis was neuroendocrine tumor of the papilla of Vater.
Conclusions: Only one case of open pancreaticoduodenectomy for PAP type 1 has been reported previously. We successfully removed a neuroendocrine tumor from the papilla of Vater in a patient with PAP type 1 through laparoscopic-assisted pancreaticoduodenectomy and detailed the operative procedures for optimal outcomes in future cases.
Keywords: laparoscopic surgical procedures; laparoscopic-assisted pancreaticoduodenectomy; pancreaticojejunostomy; portal annular pancreas; postoperative pancreatic fistula.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Karasaki H, Mizukami Y, Ishizaki A, et al. Portal annular pancreas, a notable pancreatic malformation: frequency, morphology, and implications for pancreatic surgery. Surgery 2009; 146: 515–8. - PubMed
-
- Ishigami K, Nishie A, Asayama Y, et al. The prevalence of transpancreatic common hepatic artery and coexisting variant anatomy. Clin Anat 2018; 31: 598–604. - PubMed
-
- Sugiura Y, Shima S, Yonekawa H, et al. The hypertrophic uncinate process of the pancreas wrapping the superior mesenteric vein and artery-a case report. Jpn J Surg 1987; 17: 182–5. - PubMed
-
- Joseph P, Raju RS, Vyas FL, et al. Portal annular pancreas. A rare variant and a new classification. JOP 2010; 11: 453–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials