

An evidence-based framework for postoperative surveillance of meningioma
- PMID: 40487584
- PMCID: PMC12137216
- DOI: 10.1093/nop/npae117
An evidence-based framework for postoperative surveillance of meningioma
Abstract
Background: Meningiomas frequently recur after surgery. Existing guidelines for postoperative surveillance are based on customary practices or limited data. This may result in excessive or inadequate surveillance.
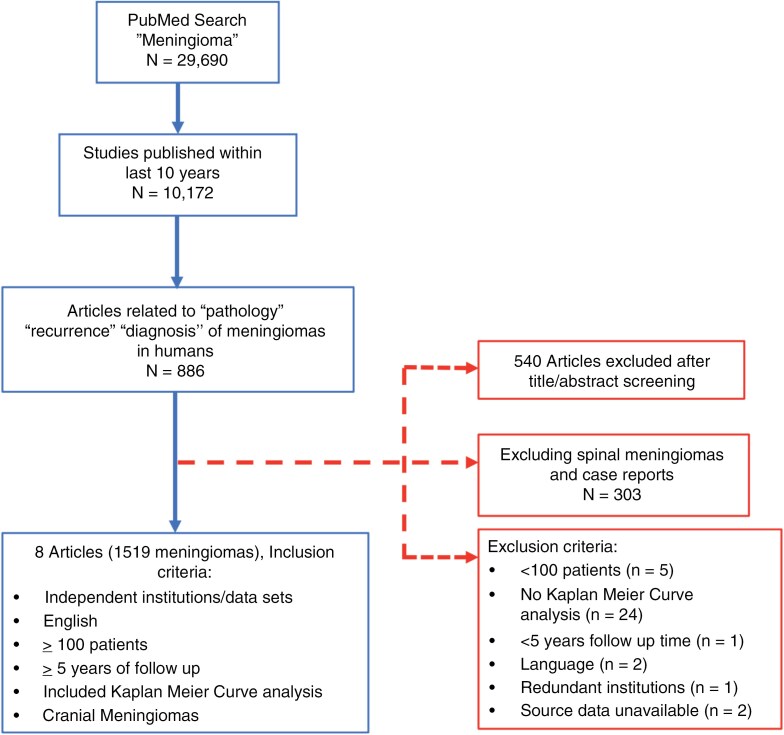
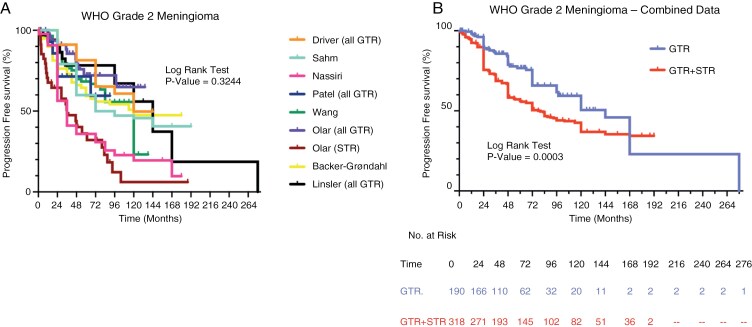
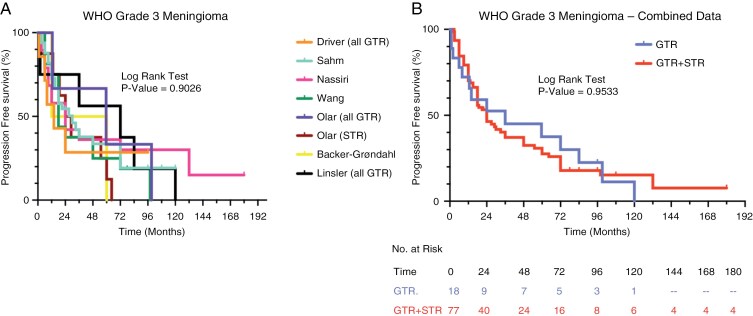
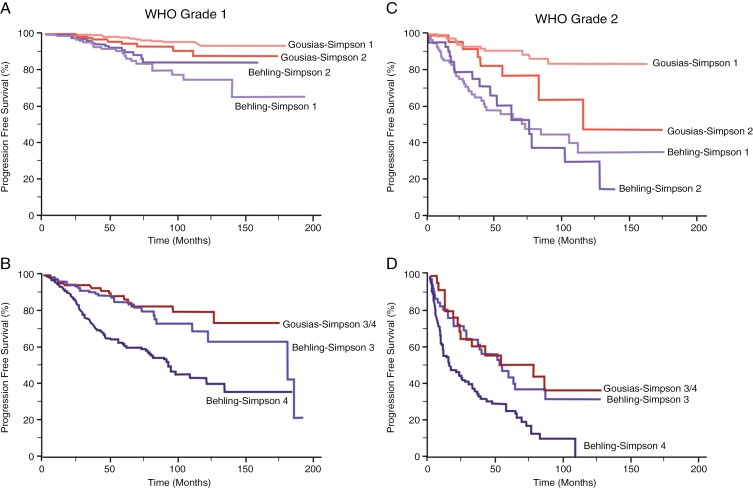
Methods: We compared 8 studies involving 1519 resected meningiomas with postoperative follow-up ranging from 7 to 23 years. Meningiomas were stratified using the World Health Organization and Simpson grading systems, and progression-free survival data were compared. Recurrence patterns were validated using 2 additional studies involving 2463 meningiomas.
Results: Incompletely resected meningiomas of all grades displayed recurrences throughout the observation period. The 5-year and 10-year cumulative incidence of recurrence for completely resected Grade 1 meningiomas was 10% and 20%, with no recurrences beyond 11 years. For completely resected Grade 2 meningiomas, the 5-year and 10-year cumulative incidence of recurrence was 24% and 50%, with ongoing recurrences throughout the observation period. Elevated recurrence rates for Grade 1/2 meningiomas persisted beyond 5 years. For completely resected Grade 3 meningiomas, the 5-year cumulative incidence of recurrence was 63%, and all recurred before 10 years.
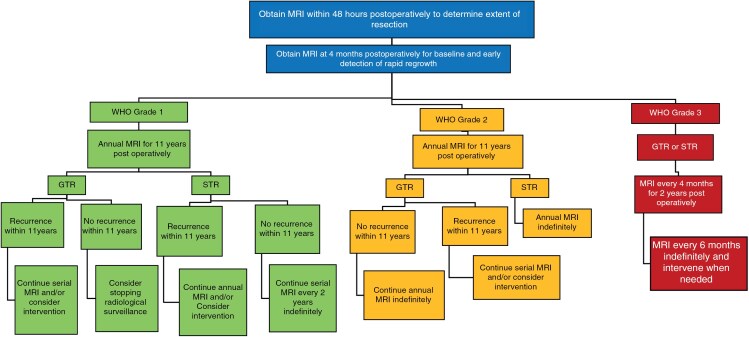
Conclusions: Postoperative magnetic resonance imaging (MRI) at 48 h to determine the extent of resection and at 4 months to detect rapid regrowth is recommended. For completely resected Grade 1 meningiomas, annual MRI followed by discontinuation of surveillance if there is no recurrence after 11 years is reasonable. For completely resected Grade 2 meningiomas, annual MRI indefinitely is recommended. For Grade 3 meningiomas, MRI every 3-4 months for 2 years, followed by every 6 months indefinitely, is recommended. Incompletely resected meningiomas should be followed indefinitely.
Keywords: follow-up; meningioma; recommendations; recurrence; surveillance.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Apra C, Peyre M, Kalamarides M.. Current treatment options for meningioma. Expert Rev Neurother. 2018;18(3):241–249. - PubMed
-
- Masalha W, Heiland DH, Franco P, et al.Atypical meningioma: progression-free survival in 161 cases treated at our institution with surgery versus surgery and radiotherapy. J Neurooncol. 2018;136(1):147–154. - PubMed
-
- Phonwijit L, Khawprapa C, Sitthinamsuwan B.. Progression-free survival and factors associated with postoperative recurrence in 126 patients with atypical intracranial meningioma. World Neurosurg. 2017;107:698–705. - PubMed
LinkOut - more resources
Full Text Sources
