

National trends in utilization and readmission following intraoperative cholangiography in gallstone pancreatitis
- PMID: 40487713
- PMCID: PMC12143823
- DOI: 10.1016/j.sopen.2025.05.002
National trends in utilization and readmission following intraoperative cholangiography in gallstone pancreatitis
Abstract
Background: In the absence of cholangitis, the role of intraoperative cholangiography (IOC) to exclude retained stones in mild gallstone pancreatitis (GSP) remains controversial. Using a nationally representative database, we examined the contemporary utilization of IOC and index outcomes and readmission following cholecystectomy for GSP.
Methods: All adults undergoing nonelective cholecystectomy for mild GSP in the 2017-2021 Nationwide Readmissions Database were identified. Patients were stratified based on the use of IOC. Multivariable regressions and Royston-Parmar analysis were used to evaluate the association of IOC use with outcomes of interest.
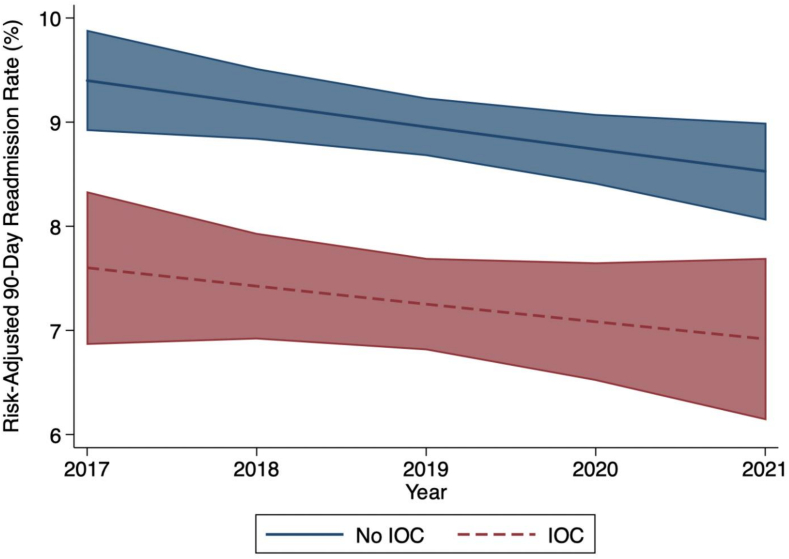
Results: Of 152,687 patients, 24.7 % underwent IOC. Utilization of IOC significantly decreased from 26.5 % to 20.7 % over the study period (p < 0.001). Compared to patients without IOC, IOC patients were older and more commonly treated at high-volume, private hospitals. Following risk adjustment, the odds of major adverse events, including mortality, complications, and bile duct injury repair were comparable between cohorts. Furthermore, length of stay and hospitalization costs were comparable between patients with and without IOC. Notably, IOC was significantly associated with 20 % decreased odds of 90-day readmission for recurrent pancreatitis or retained stone, which persisted over time (AOR 0.80 [95 % CI 0.74-0.86]).
Conclusions: IOC was associated with significantly reduced readmission and comparable resource use following cholecystectomy for GSP. Despite its decreasing utilization, IOC may be a cost-effective strategy to help reduce risk for recurrent biliary disease among patients with mild GSP.
Keywords: Bile duct; Cholecystectomy; Gallstone pancreatitis; Intraoperative cholangiography; Outcomes; Readmission.
© 2025 The Authors.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





References
-
- McNabb-Baltar J., Ravi P., Isabwe G.A., et al. A population-based assessment of the burden of acute pancreatitis in the United States. Pancreas. 2014;43(5):687–691. - PubMed
-
- Acosta J.M., Ledesma C.L. Gallstone migration as a cause of acute pancreatitis. N Engl J Med. 1974;290(9):484–487. - PubMed
-
- Hwang S.S., Li B.H., Haigh P.I. Gallstone pancreatitis without cholecystectomy. JAMA Surg. 2013;148:867–872. - PubMed
-
- Da Costa D.W., Bouwense S.A., Schepers N.J., et al. Same-admission versus interval cholecystectomy for mild gallstone pancreatitis (PONCHO): a multicentre randomised controlled trial. Lancet. 2015;386:1261–1268. - PubMed
LinkOut - more resources
Full Text Sources
