

Risk factors associated with low bone mineral density and childhood osteoporosis in a population undergoing skeletal growth: a cross-sectional analytic study
- PMID: 40487764
- PMCID: PMC12141024
- DOI: 10.3389/fendo.2025.1587985
Risk factors associated with low bone mineral density and childhood osteoporosis in a population undergoing skeletal growth: a cross-sectional analytic study
Abstract
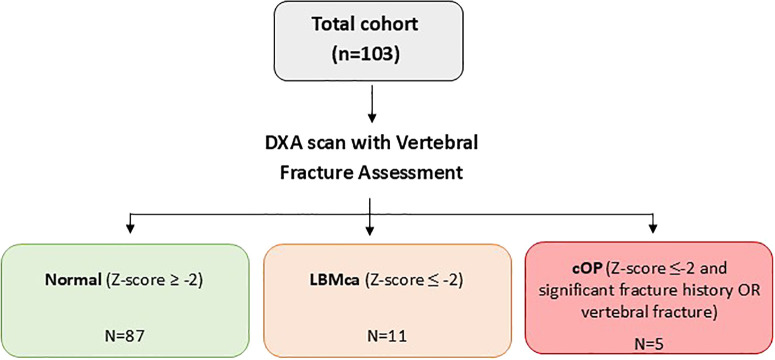
Background: Early identification of risk factors for low bone mass for chronological age (LBMca) and childhood osteoporosis (cOP) in patients undergoing skeletal growth is essential to mitigate long-term skeletal complications. cOP is diagnosed when LBMca (BMD Z-score ≤2) is accompanied by a clinically significant fracture history, or when vertebral fragility fractures are present.
Methods: Patients under 21 years of age with at least one risk factor for LBMca (malabsorption syndrome, chronic inflammatory diseases, hematological diseases, endocrinopathies, drugs that affect bone metabolism, or insufficient calcium intake) were included. Data on fractures history and physical activity levels were collected. Spine and whole-body dual-energy x-ray absorptiometry (DXA) and vertebral morphometry were performed. Age-adjusted linear regression analysis evaluated associations between bone mineral density (BMD) and risk factors.
Results: A total of 103 patients were included (mean age 9.8 years; 52.4% female), and 96.1% had more than two risk factors. The prevalence of LBMca was 10.5% and the prevalence of cOP was 4.8%. Vertebral BMD was positively associated with male sex. Whole body BMD was negatively associated with sedentary lifestyle and fracture history. Total body less head BMD showed negative associations with current steroid treatment, sedentary lifestyle, and history of fractures.
Conclusions: Pediatric populations at risk of LBMca or cOP often have multiple risk factors, notably modifying ones such as physical inactivity. Up to 10.5% of children with risk factors present LBMca and 4.8% have an undiagnosed or unknown cOP. Longitudinal studies are warranted to understand the long-term impact of the identified risk factors, including age, sex, sedentary lifestyle, ethnicity and vitamin D status, on bone health.
Keywords: DXA (dual-energy x-ray absorptiometry); bone fragility; bone mineral density; childhood osteoporosis; low bone mass for chronological age.
Copyright © 2025 Magallares, Cerdá, Betancourt, Fraga, Park, Codes-Méndez, Quesada-Masachs, López-Corbeto, Torrent, Marín, Herrera, Gich, Boronat, Casademont, Corominas and Malouf.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Pitukcheewanont P, Austin J, Chen P, Punyasavatsut N. Bone health in children and adolescents: risk factors for low bone density. Pediatr Endocrinol Rev: PER. (2013) 10:318–35. - PubMed
-
- S B. Osteoporosis infantil. Protoc Diagn Ter Pediatr. (2014) 1:197–201.
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical