

Acute medullary ischemia as clinical presentation of an intact infrarenal abdominal aortic aneurysm
- PMID: 40488186
- PMCID: PMC12141886
- DOI: 10.1016/j.jvscit.2025.101805
Acute medullary ischemia as clinical presentation of an intact infrarenal abdominal aortic aneurysm
Abstract
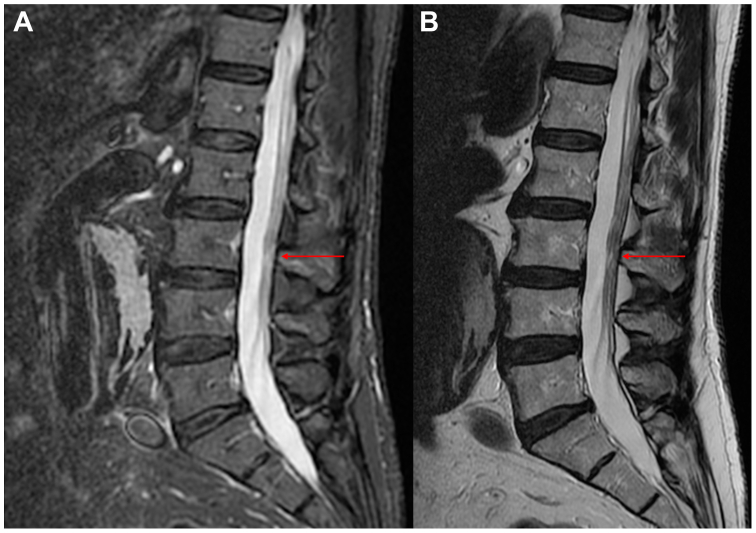
Abdominal aortic aneurysms (AAAs) are usually asymptomatic. Abdominal and/or low back pain are signs of rupture or impending rupture. We report the case of an 88-year-old man with unusual symptoms of clinical presentation for an AAA. He was admitted to our hospital with low back pain associated with bilateral lower extremity paresis. Examination revealed an abdominal pulsatile mass, and palpable peripheral pulses. Computed tomography angiography detected a 65-mm intact infrarenal AAA with neither signs of fissure or rupture nor lower extremity arterial disease. Magnetic resonance imaging demonstrated low-intensity signals at L1-L2 in the middle of the conus medullaris (acute medullary ischemia). The patient was managed conservatively with monoantiplatelet therapy, and low-weight-molecular heparin. Symptoms were resolved completely after 3 days. The final decision was to not treat the AAA.
Keywords: Abdominal aortic aneurysm; Acute medullary ischemia; Spinal cord ischemia.
© 2025 The Author(s).
Conflict of interest statement
None.
Figures

References
-
- Lee H., Papanagnou D., Berman M., Zhang X.C. Man with sudden paralysis: insidious spinal cord infarction due to a non-ruptured abdominal aortic aneurysm. J Emerg Med. 2019;56:413–416. - PubMed
-
- Sveinsson O., Elmi-Terander A., Edström E., Andersson M., Stenimahitis V. Spinal cord infarction - a rare condition and a diagnostic challenge. Lakartidningen. 2021;118 - PubMed
-
- Moulakakis K.G., Alexiou V.G., Karaolanis G., et al. Spinal cord ischemia following elective endovascular repair of infrarenal aortic aneurysms: a systematic review. Ann Vasc Surg. 2018;52:280–291. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
