

Diagnostic accuracy of symptoms compared to endoscopy, biopsy and bile reflux index in detecting reflux-related abnormalities at one year after OAGB
- PMID: 40488857
- PMCID: PMC12149249
- DOI: 10.1007/s00423-025-03748-y
Diagnostic accuracy of symptoms compared to endoscopy, biopsy and bile reflux index in detecting reflux-related abnormalities at one year after OAGB
Abstract
Background: The diagnostic accuracy of clinical symptoms in detecting reflux-related abnormalities after One anastomosis gastric Bypass (OAGB) remains unclear. This study evaluates the diagnostic performance of reflux symptoms compared to upper endoscopy (UE), biopsy, and bile reflux index (BRI) findings at one-year post-OAGB.
Methods: A retrospective analysis was conducted on 150 consecutive patients who underwent OAGB between November 2017 and June 2018 and had no preoperative reflux symptoms. At one year postoperatively, patients completed the Gastroesophageal Reflux Disease Questionnaire (GerdQ) for symptom assessment. UE, histopathological biopsy, and BRI calculations were performed. The diagnostic accuracy of symptoms was evaluated against UE, biopsy, and BRI findings using sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the area under the receiver operating characteristic curve (AUROC).
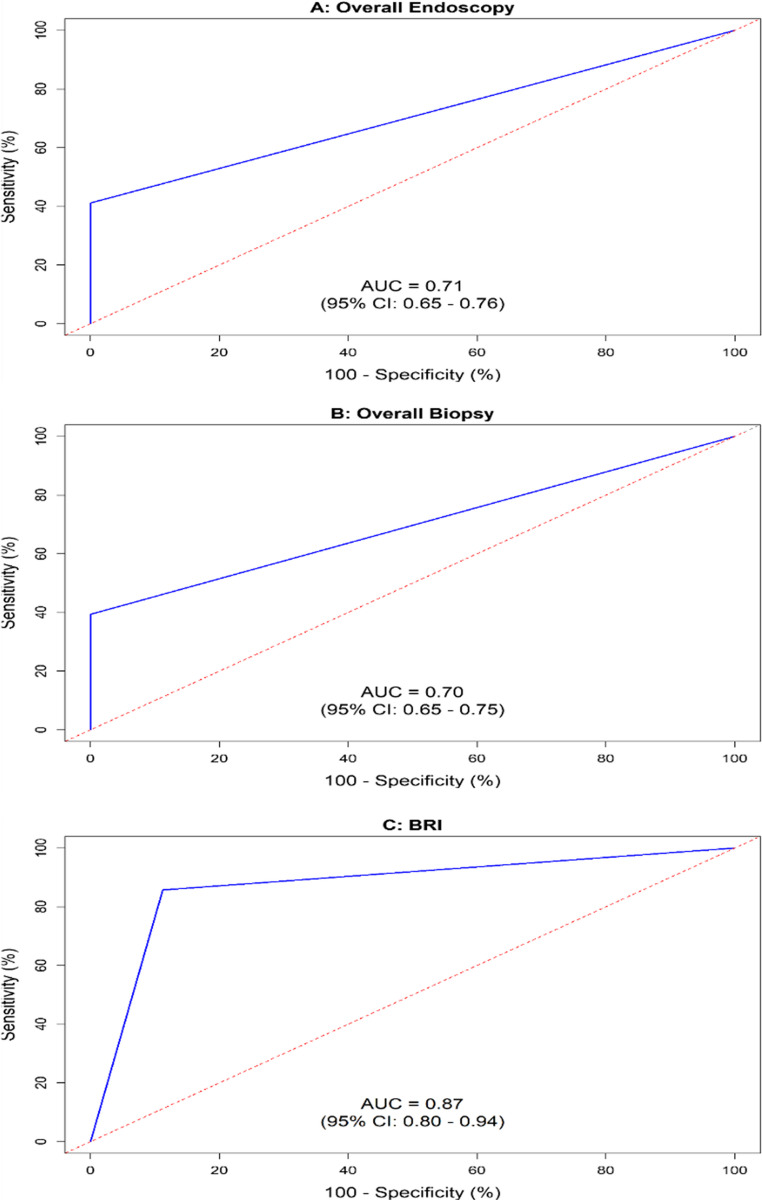
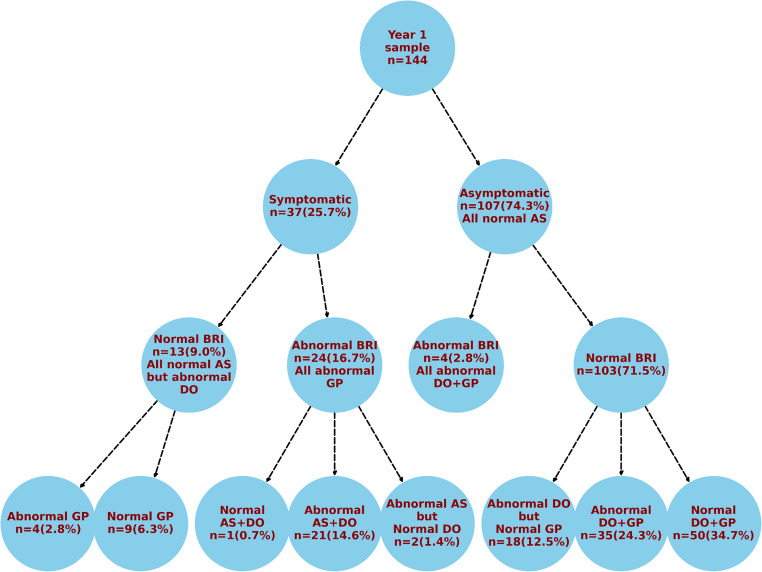
Results: Among 144 patients analyzed, 25.7% reported GERD symptoms, while abnormal findings were observed in 62.5% (UE), 65.3% (biopsy), and 19.4% (BRI). Symptoms demonstrated high specificity and PPV (100%) in predicting UE and biopsy abnormalities but had low sensitivity (41.1% for UE, 39.4% for biopsy) and moderate NPVs (50.5% and 46.7%, respectively), indicating a risk of false negatives. The AUROC values were 0.71 (UE) and 0.70 (biopsy), reflecting moderate diagnostic discrimination. For BRI, symptom presence had 88.8% specificity and 64.9% PPV, but symptom absence correlated with high sensitivity (85.7%) and excellent NPV (96.3%), yielding an AUC of 0.87. Notably, 95.8% of symptomatic patients with abnormal BRI exhibited anastomotic site abnormalities, and 95.7% of patients with anastomotic pathology had concurrent distal esophageal and gastric pouch abnormalities.
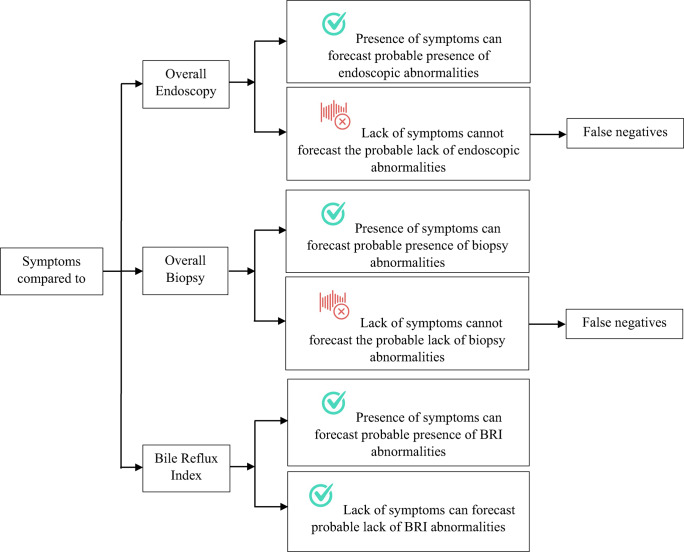
Conclusions: Symptoms may serve as a predictor of reflux-related abnormalities on UE or biopsy, but their absence is unreliable in ruling out such abnormalities. While symptoms effectively forecast abnormal BRI in high-prevalence settings, their diagnostic utility remains limited. Further research is warranted to assess long-term diagnostic accuracy and refine post-OAGB reflux assessment protocols.
Keywords: Biopsy; Diagnostic accuracy; Endoscopy; GERD; OAGB; Reflux; Symptoms.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was approved by the Ethics Committees at the institution where the study was implemented. Informed consent: Written informed consent was provided by each patient who participated in the study. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Reflux-Related Abnormalities at Distal oesophagus, Gastric Pouch and Anastomotic Site 4 Years After OAGB: Diagnostic Accuracies of Endoscopy Compared to Biopsy and of Symptoms Compared to Both.Obes Surg. 2025 Apr;35(4):1273-1284. doi: 10.1007/s11695-025-07700-3. Epub 2025 Mar 14. Obes Surg. 2025. PMID: 40087244
-
Evaluation of esophageal pathology in a group of patients 2 years after one-anastomosis gastric bypass (OAGB) - Cohort study.Obes Res Clin Pract. 2022 Jan-Feb;16(1):82-86. doi: 10.1016/j.orcp.2021.12.001. Epub 2021 Dec 16. Obes Res Clin Pract. 2022. PMID: 34922847
-
Bile Reflux is a Common Finding in the Gastric Pouch After One Anastomosis Gastric Bypass.Obes Surg. 2020 Mar;30(3):875-881. doi: 10.1007/s11695-019-04353-x. Obes Surg. 2020. PMID: 31853864 Free PMC article. Clinical Trial.
-
Randomized Controlled Trial of One Anastomosis Gastric Bypass Versus Roux-En-Y Gastric Bypass for Obesity: Comparison of the YOMEGA and Taiwan Studies.Obes Surg. 2019 Sep;29(9):3047-3053. doi: 10.1007/s11695-019-04065-2. Obes Surg. 2019. PMID: 31290104 Review.
-
One Anastomosis Gastric Bypass and Risk of Cancer.Obes Surg. 2018 May;28(5):1441-1444. doi: 10.1007/s11695-018-3156-5. Obes Surg. 2018. PMID: 29516398 Review.
References
-
- El Ansari W, Elhag W (2022) Preoperative prediction of body mass index of patients with type 2 diabetes at 1 year after laparoscopic sleeve gastrectomy: cross-sectional study. Metab Syndr Relat Disord 20(6):360–366. 10.1089/met.2021.0153 - PubMed
-
- Elgenaied I, El Ansari W, Elsherif MA, Abdulrazzaq S, Qabbani AS, Elhag W (2020) Factors associated with complete and partial remission, improvement, or unchanged diabetes status of obese adults 1 year after sleeve gastrectomy. Surg Obes Relat Dis 16(10):1521–1530. 10.1016/j.soard.2020.05.013 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
