

Long-term bleeding events post-percutaneous coronary intervention in patients with malignancy with and without anticoagulant therapy
- PMID: 40489022
- PMCID: PMC12431914
- DOI: 10.1007/s12928-025-01151-4
Long-term bleeding events post-percutaneous coronary intervention in patients with malignancy with and without anticoagulant therapy
Abstract
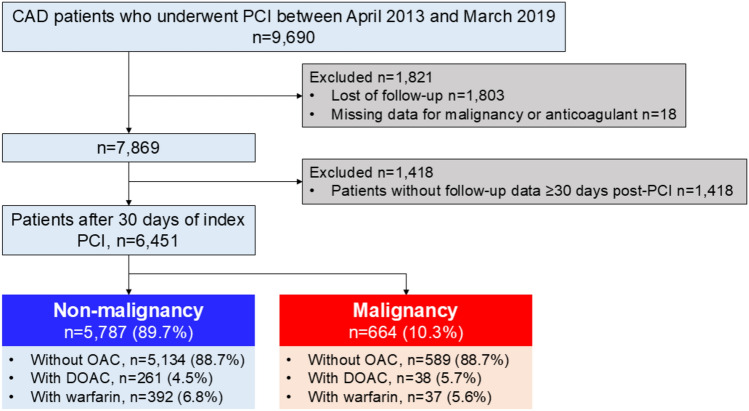
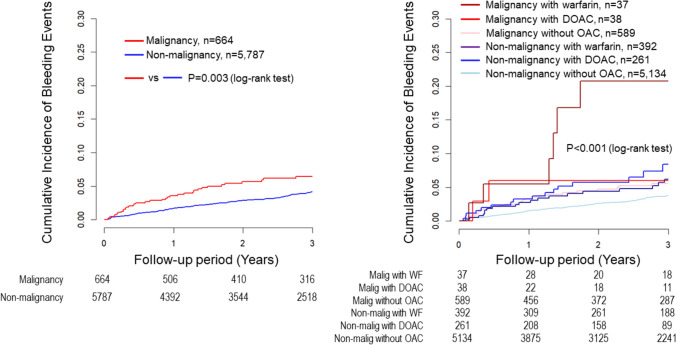
The prevalence of malignancies in patients undergoing percutaneous coronary intervention (PCI) is increasing with aging. Active malignancy is a significant contributor to high bleeding risk. For cancer patients requiring oral anticoagulant (OAC) therapy, the choice between direct oral anticoagulants (DOAC) and warfarin is critical. The aim of this study was to investigate long-term bleeding events in patients with malignancy undergoing PCI. The CLIDAS (Clinical Deep Data Accumulation System) multicenter database includes data from seven tertiary medical hospitals in Japan. This retrospective analysis included 6451 patients who underwent PCI between April 2013 and March 2019 and completed 3-year follow-up. The patients were divided into two groups; No malignancy (n = 5787) and Malignancy group (n = 664). Malignancy was defined by a history of cancer treatment. These groups were further subcategorized based on OAC therapy; (1) No malignancy without OAC (n = 5134), (2) No malignancy with DOAC (n = 261), (3) No malignancy with warfarin (n = 392), (4) Malignancy without OAC (n = 589), (5) Malignancy with DOAC (n = 38), and (6) Malignancy with warfarin (n = 37). The primary outcome was the incidence of bleeding events, defined according to the Global Use of Streptokinase and t-PA for Occluded Coronary Arteries classification of moderate and severe bleeding. The secondary outcomes were major adverse cardiac events (MACE) and net adverse clinical events (NACE). Multivariable Cox regression analysis showed that the malignancy with warfarin group had a significantly higher risk of bleeding events compared to the malignancy without OAC group (hazard ratio [HR], 3.64; 95% confidence interval [CI], 1.38-9.61, p value = 0.009). No significant differences were observed for MACE (HR, 1.39; 95% CI 0.59-3.25, p value = 0.454) or NACE (HR, 1.62; 95% CI, 0.80-3.29; p value = 0.184). Malignancy patients receiving warfarin were associated with a higher risk of bleeding events. DOACs may represent a preferable alternative to warfarin with regard to bleeding risk in patients with malignancy undergoing PCI.
Keywords: High bleeding risk; Malignancy; PCI.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: TM received research grants from Amgen and honoraria from Abbott Medical and Bayer. T Kabutoya received scholarship funding from Abbott Medical and the Joint Research Fund of Novartis Pharmaceutical. YI received honoraria from Daiichi Sankyo and Toa Eiyo, Japan. KK received research grants and honoraria from Sanwa Kagaku and Kenkyusho. AK received honoraria from AstraZeneca, Eli Lilly, and Sumitomo Pharma. YN received research grants and consultations from Bayer. KT received remuneration for lectures from Abbott Medical Co., Ltd., Amgen K.K., Bayer Yakuhin, Ltd., Daiichi Sankyo Co., Ltd., Kowa Pharmaceutical Co. Ltd., Nippon Boehringer Ingelheim Co., Ltd., Novartis Pharma K.K., Otsuka Pharmaceutical Co., Ltd., Pfizer Japan Inc., Takeda Pharmaceutical Co., Ltd., and TERUMO Co, Ltd.; trust research/joint research funds from Bayer Yakuhin, Ltd., Bristol-Myers K.K., Daiichi Sankyo Co., Ltd., MOCHIDA PHARMACEUTICAL CO., LTD., EA Pharma Co., Ltd., TAUNS Laboratories, Inc., Novo Nordisk Pharma Ltd., and PRA Health Sciences; received scholarship funds from Abbott Medical Co., Ltd., ITI Co.,Ltd., Boehringer Ingelheim Japan, Otsuka Pharmaceutical Co., Ltd., and Boston Scientific Japan K.K; and was affiliated with endowed departments at Abbott Japan Co., Ltd., Boston Scientific Japan K.K., Fides-one, Inc., GM Medical Co., Ltd., ITI Co., Ltd., Kaneka Medix Co., Ltd., NIPRO CORPORATION, TERUMO Co, Ltd., Philips Japan Ltd., Getinge Group Japan K.K., Orbusneich Medical K. K., Abbott Medical Co., Ltd., BIOTRONIK JAPAN, INC., Boston Scientific Japan K.K., Fukuda Denshi Co., Ltd., Japan Lifeline Co., Ltd., Medtronic Japan Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., and NIPRO CORPORATION. HS reported stocks and stock options with precision. HF received consulting fees from Mehergen Group Holdings and honoraria from Novartis Pharma and Otsuka Pharmaceutical. RN received research grants from Novartis Pharma K.K. and honoraria for lecture from Kowa Company. The authors declare no conflict of interest. Ethical approval: This study was approved by the Institutional Review Board of Kumamoto University Hospital (Senshin-No. 2406) and each institutional ethics committee, and was in accordance with the Declaration of Helsinki. This study was waived from the requirement for individual informed consent because all data were anonymized by the participating institutions and were then collected in the CLIDAS database.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
