

Active Travel Mode and Incident Dementia and Brain Structure
- PMID: 40489111
- PMCID: PMC12150188
- DOI: 10.1001/jamanetworkopen.2025.14316
Active Travel Mode and Incident Dementia and Brain Structure
Abstract
Importance: Active travel modes, such as walking and cycling, are feasible and readily embraced forms of physical activity, but their association with dementia risk and brain structure remains unclear.
Objectives: To investigate the long-term association between travel modes and dementia risk and brain structural metrics and to evaluate whether genetic predisposition could modify the association between travel modes and dementia risk.
Design, setting, and participants: This prospective cohort study included data collected from the UK Biobank from March 13, 2006, to October 1, 2010. Data were analyzed from March to October 2024.
Exposures: Travel modes assessed using the question "In the last 4 weeks, which forms of transport have you used most often to get about (not including any journeys to and from work)?" and categorized into 4 groups: nonactive, walking, mixed-walking, and cycling and mixed-cycling mode.
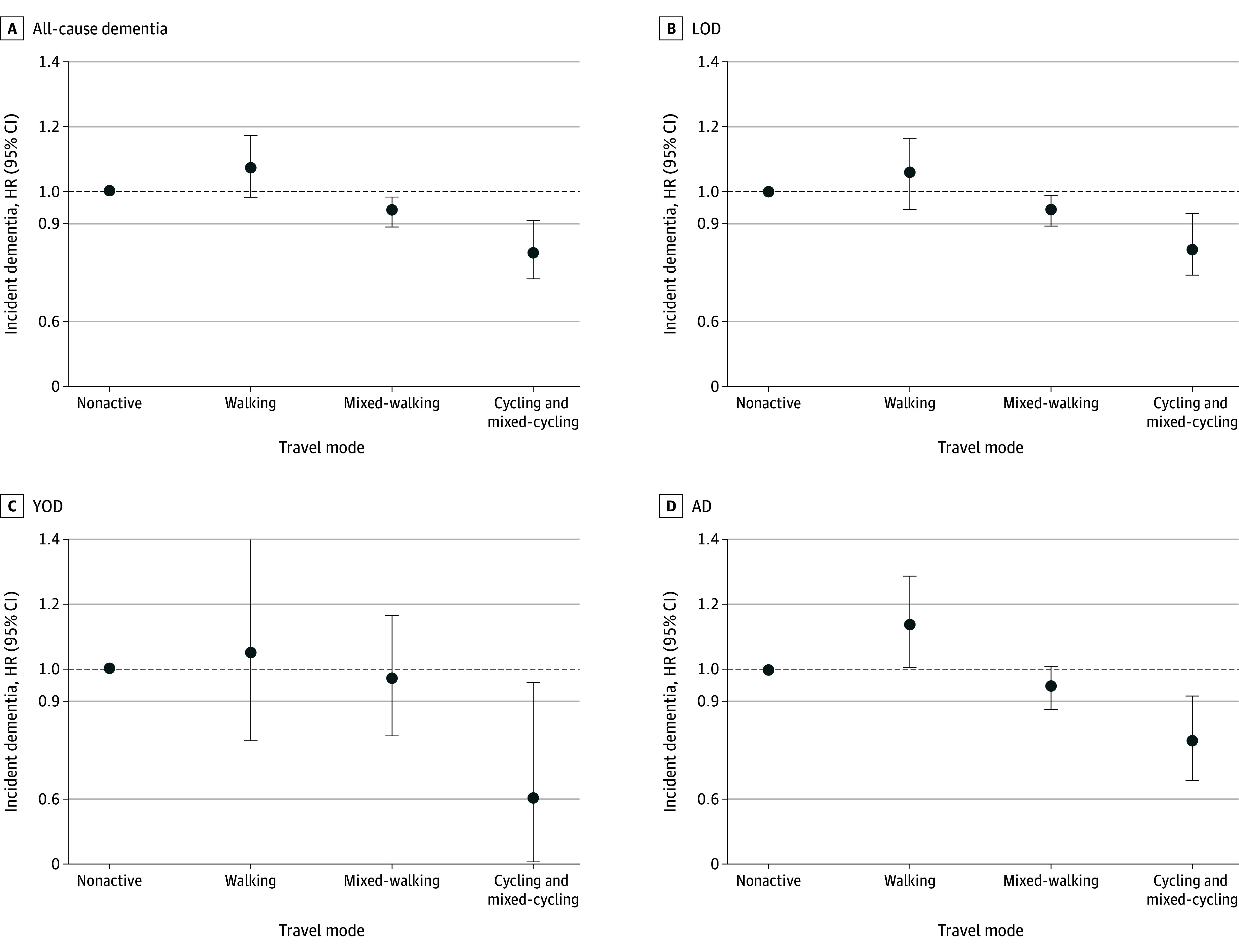
Main outcomes and measures: The incidence of all-cause dementia (including young-onset dementia [YOD] and late-onset dementia [LOD]) was the primary outcome, and dementia subtypes, such as Alzheimer disease (AD) and brain structure, were the secondary outcomes; all were identified through hospital records and death registers. Brain structure was measured by a magnetic resonance imaging scan. Travel mode and risk of incident dementia were assessed using Cox proportional hazards regression models with hazard ratios and 95% CIs.
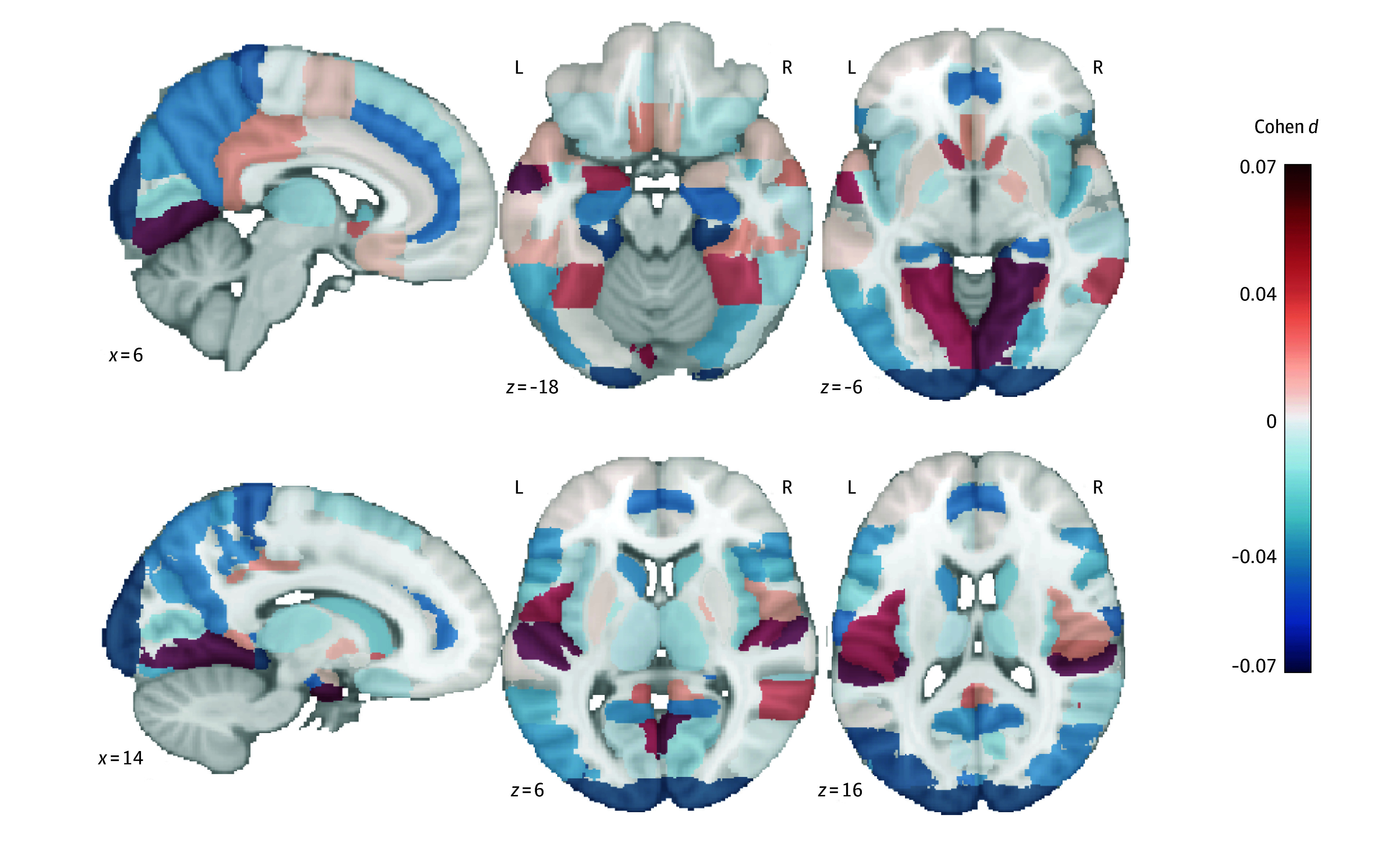
Results: The study encompassed 479 723 participants (mean [SD] age, 56.5 [8.1] years; 260 730 females [54.4%]), including 271 690 in the YOD analyses and 334 939 in the LOD analyses. Over a median follow-up of 13.1 years (IQR, 12.8-13.5 years), 8845 cases of dementia (1.8%) and 3956 cases of AD (0.8%) were recorded. Compared with a nonactive travel mode, multivariable-adjusted hazard ratios for cycling and mixed-cycling were 0.81 (95% CI, 0.73-0.91) for all-cause dementia, 0.78 (95% CI, 0.66-0.92) for AD, 0.60 (95% CI, 0.38-0.95) for YOD, and 0.83 (95% CI, 0.75-0.93) for LOD. A significant interaction between travel mode and genetic susceptibility in the all-cause dementia analysis (P = .02 for interaction) and the LOD analysis (P = .04 for interaction) was observed; specifically, for the cycling and mixed-cycling groups, the risks of all-cause dementia and LOD were lower among those without apolipoprotein E ε4 (APOE ε4) carrier status (all-cause dementia: hazard ratio [HR], 0.74 [95% CI, 0.63-0.87]; LOD: HR, 0.75 [95% CI, 0.63-0.89]) compared with those with APOE ε4 carrier status (all-cause dementia: HR, 0.88 [95% CI, 0.76-1.02]; LOD: HR, 0.91 [95% CI, 0.78-1.05]). The cycling and mixed-cycling mode was significantly associated with a higher hippocampal volume (β, 0.05 [95% CI, 0.02-0.08]). Genetic risk significantly modified the association with all-cause dementia (P = .02 for interaction) and LOD (P = .04 for interaction). Specifically, for the cycling and mixed-cycling groups, the risk of all-cause dementia was lower among those without APOE ε4 (HR, 0.74 [95% CI, 0.63-0.87]) compared with those with APOE ε4 (HR, 0.88 [95% CI, 0.76-1.02]). Similarly, the risk of LOD was lower among those without APOE ε4 (HR, 0.75 [95% CI, 0.63-0.89]) compared with those with APOE ε4 (HR, 0.91 [95% CI, 0.78-1.05]).
Conclusions and relevance: The findings of this cohort study suggest an association between active travel mode and incident dementia and brain structure. The cycling and mixed-cycling mode was associated with a reduced risk of all-cause dementia, including YOD, LOD, and AD, as well as an increased hippocampal volume, suggesting a promising approach for maintaining brain health.
Conflict of interest statement
Figures
Similar articles
-
Associations Between Walking Pace, APOE-ε4 Genotype, and Brain Health in Middle-Aged to Older Adults.Med Sci Sports Exerc. 2025 Jun 1;57(6):1212-1220. doi: 10.1249/MSS.0000000000003646. Epub 2025 Jan 9. Med Sci Sports Exerc. 2025. PMID: 39780372
-
Walking pace, handgrip strength, age, APOE genotypes, and new-onset dementia: the UK Biobank prospective cohort study.Alzheimers Res Ther. 2023 Jan 9;15(1):9. doi: 10.1186/s13195-022-01158-6. Alzheimers Res Ther. 2023. PMID: 36624486 Free PMC article.
-
Association between active commuting and incident cardiovascular disease, cancer, and mortality: prospective cohort study.BMJ. 2017 Apr 19;357:j1456. doi: 10.1136/bmj.j1456. BMJ. 2017. PMID: 28424154
-
Exposure to air pollution and risk of incident dementia in the UK Biobank.Environ Res. 2022 Jun;209:112895. doi: 10.1016/j.envres.2022.112895. Epub 2022 Feb 8. Environ Res. 2022. PMID: 35149105 Free PMC article.
-
Association of apolipoprotein E genetic variation in Alzheimer's disease in Indian population: a meta-analysis.Am J Alzheimers Dis Other Demen. 2014 Nov;29(7):575-82. doi: 10.1177/1533317514531443. Am J Alzheimers Dis Other Demen. 2014. PMID: 25551132 Free PMC article. Review.
References
-
- Alzheimer’s Disease International . World Alzheimer report 2023. September 21, 2023. Accessed July 14, 2024. https://www.alzint.org/resource/world-alzheimer-report-2023/
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
