

Outcomes After Thrombectomy for Acute Ischemic Stroke Related to Type of Stent Retriever; a MR CLEAN Registry Study
- PMID: 40490624
- PMCID: PMC12325387
- DOI: 10.1007/s00270-025-04048-0
Outcomes After Thrombectomy for Acute Ischemic Stroke Related to Type of Stent Retriever; a MR CLEAN Registry Study
Abstract
Purpose: Endovascular treatment (EVT) with a stent retriever is known to be effective and safe in patients with acute ischemic stroke due to large vessel occlusion. We aimed to compare the most used stent retrievers in a nationwide registry of EVT-treated stroke patients (MR CLEAN Registry).
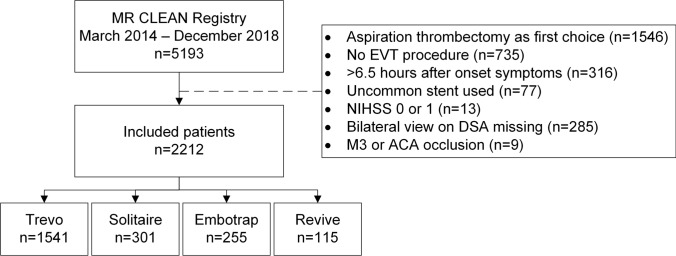
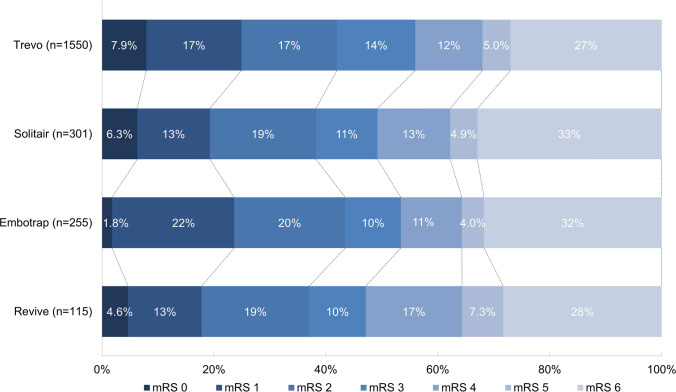
Methods: Patients with ischemic stroke due to large vessel occlusion, treated with stent retriever thrombectomy (each stent retriever with at least 100 EVTs) as first-line technique in the MR CLEAN Registry, were included. The primary outcome was the modified Rankin Scale (mRS) score at 90-day follow-up. Secondary outcomes included reperfusion (expanded Treatment In Cerebral Infarction [eTICI]), mortality at 90 days, symptomatic intracranial hemorrhage, National Institutes of Health Stroke Scale (NIHSS) score between 24 and 48 h post-EVT, and procedure time. With multivariable regression analyses, we calculated odds ratios (OR) and β-estimates to compare outcomes between the most frequently used stent retrievers, with adjustments for predefined variables. One subgroup analysis focused on the effect of the stent retriever on outcomes in M1 occlusions.
Results: Trevo (Stryker) was the most frequently used stent retriever (n = 1541, 70%). Other types were Solitaire (n = 301, 14%) (Medtronic), Embotrap (n = 255, 11%) (Cerenovus; Johnson&Johnson), and Revive (n = 103, 5.2%) (Cerenovus; Johnson&Johnson). There was a slightly, but statistically significant, higher 90-day mRS score (adjusted common [ac]OR: 0.75, 95%CI: 0.57-0.99) and mortality rate (aOR: 1.77, 95%CI: 1.16-2.68) for the Solitaire and longer procedure times for the Revive stent (mean: 67.6 versus 58.9 min; adjusted β-estimate: 11.6, 95%CI: 2.69-20.6) compared to the Trevo retriever. There were no outcome differences in the M1 subgroup analyses.
Conclusion: Differences in clinical, technical, and safety outcomes after EVT between the Trevo, Solitaire, Embotrap, and Revive stent retrievers were-although statistically significant-small. Treating physicians should use the stent retriever they are used to, and further studies with more strict patient selection should be conducted to validate these results.
Keywords: Endovascular treatment (EVT); Stent retriever (SR); Stroke; Thrombectomy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: BJE reports funding from the Netherlands Organisation for Health Research and Development and Health Holland Top Sector Life Sciences & Health, and unrestricted Grants from Nicolab, all paid to institution. MU reports research grants From the Dutch Heart Foundation, the Netherlands Organisation for Health Research and Development, and Belgian Health Care Knowledge Centre (all paid to institution); and support to attend the Stroke Symposium Johnson & Johnson 2022. CBLMM reports grants from the Netherlands Cardiovascular Research Initiative, an initiative of the Dutch Heart Foundation, TWIN Foundation, European Commission, Healthcare Evaluation Netherlands, and Stryker (all paid to institution); and is a (minority interest) shareholder of Nicolab. YBWEMR reports being a minor shareholder of Nicolab. AvdL reports grants from Stryker, Thrombolytic Science, Penumbra, GE Healthcare, Philips Healthcare, and Siemens Healthineers (all paid to institution); reports payments from Siemens Healthineers (all paid to institution); participates in the advisory board of ESCAPE-MEVO; and is a research leader of the CONTRAST consortium. DWJD reports funding from the Dutch Heart Foundation, Netherlands Brain Foundation, the Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, Penumbra, Stryker, Medtronic, Thrombolytic Science, and Cerenovus (all unrestricted grants for research), paid to institution. WHvZ reports speaker fees from Stryker, Cerenovus, and Nicolab, and consulting fees from Philips (all paid to institution); participated in the advisory boards of WeTrust (Philips) and ANAIS (Anaconda) (all paid to institution); and participated in the advisory boards of InEcxtremis (CHU Montpellier, Montpellier, France) and DISTAL (University Hospital Basel, Basel, Switzerland), studies for which no payments were received. All other authors declare no competing interests. Ethical Approval: For this type of study, formal consent is not required. Informed Consent: The MR CLEAN Registry study protocol was granted with the permission to carry out the study as a registry after evaluating by the medical ethics committee of the Erasmus University Medical Center (MEC-2014–235). The committee waived the need for obtaining informed consent. Consent for Publication: For this type of study, consent for publication is not required.
Figures
References
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372(1):11–20. - PubMed
-
- Badhiwala JH, Nassiri F, Alhazzani W, Selim MH, Farrokhyar F, Spears J, et al. Endovascular thrombectomy for acute ischemic stroke: a meta-analysis. JAMA. 2015;314(17):1832–43. - PubMed
-
- Munich SA, Vakharia K, Levy EI. Overview of Mechanical Thrombectomy Techniques. Neurosurgery. 2019;85(suppl_1):S60-S7. - PubMed
-
- Pierot L, Soize S, Benaissa A, Wakhloo AK. Techniques for endovascular treatment of acute ischemic stroke: from intra-arterial fibrinolytics to stent-retrievers. Stroke. 2015;46(3):909–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
