

Ovarian remnant syndrome: an unsuspected diagnosis
- PMID: 40491391
- PMCID: PMC12233126
- DOI: 10.52054/FVVO.2025.49
Ovarian remnant syndrome: an unsuspected diagnosis
Abstract
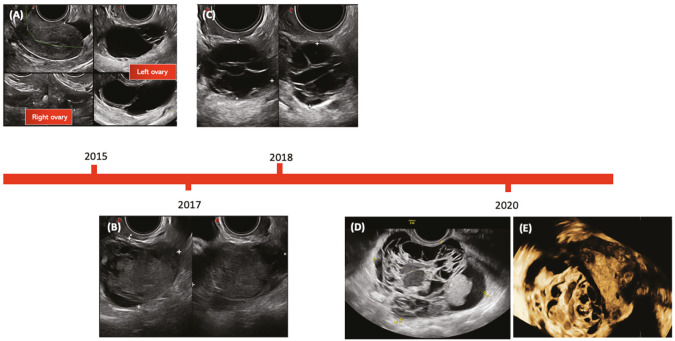
Background: Ovarian remnant syndrome (ORS) is a rare condition defined by the presence of residual tissue of ovarian origin, histologically confirmed in a woman with a previous salpingo-oophorectomy, usually as a result of difficult surgery in the presence of adhesions.
Objectives: To evaluate the existing literature on ORS.
Methods: A narrative review was performed. A search for relevant articles was carried out in PubMed for the period from January 2014 to July 2024. Three original cases of ORS are also reported.
Main outcome measures: All available literature on the subject was analysed and articles relevant to the topic of the review were included. Additional articles were reviewed to provide an overview of the issue.
Results: A total of 10 different cases of ORS found in the literature were analysed, together with 3 original cases.
Conclusions: The presence of distorted anatomy and extensive adhesions may lead to an increased risk of residual ovarian tissue. Residual ovarian tissue may sometimes evolve into a malignant lesion. When difficult oophorectomy is suspected, the surgeon must proceed with caution to complete oophorectomy. Strict follow-up is essential to detect ORS.
What is new?: This is the first narrative review including cases described in the literature and three new original cases. Our work provides a comprehensive and global view of this condition and may help in clinical practice to reduce the risk of ORS through appropriate surgical planning and possibly early diagnosis of the syndrome.
Keywords: Ovarian remnant syndrome; endometrioid ovarian carcinoma; ultrasound.
Conflict of interest statement
Figures




References
-
- Vilos GA, Marks-Adams JL, Vilos AG, Oraif A, Abu-Rafea B, Casper RF. Medical treatment of ureteral obstruction associated with ovarian remnants and/or endometriosis: report of three cases and review of the literature. J Minim Invasive Gynecol. 2015;22(3):462–8. doi: 10.1016/j.jmig.2014.12.153. - DOI - PubMed
LinkOut - more resources
Full Text Sources